Keywords
Cohort Studies; Incidence; Pancreatic Neoplasms; Venous Thromboembolism
Abbreviations
ESA: Erythropoietin-stimulating agents; LMWH: Low Molecular weight Heparin; PSGL-1 VNRT: Platelet-Selectin Glycoprotein Ligand-1 variable number of tandem repeats; VTE: Venous thromboembolism
What We Knew Before 2014 ASCO Annual Meeting?
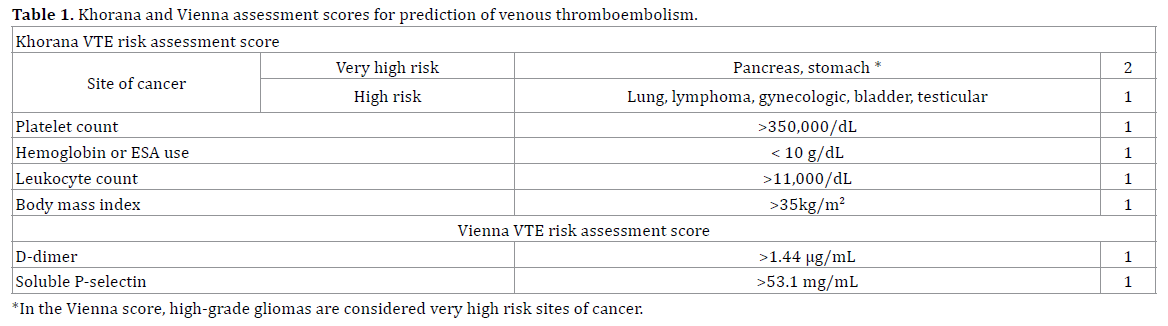
Venous thromboembolism is the second leading cause of death in cancer patients [1]. The incidence of venous thromboembolism in oncologic patients 3 months after starting chemotherapy isapproximately7% (range 4.6%- 11.6% across cancer locations) and then rising to 13.5% at 12 months (range 9.8%-21.3%) with the highest venous thromboembolism risk associated with pancreatic, stomach, and lung cancer [2].The incidence of VTE reaches 20% or more in pancreatic cancer and metastatic glioblastoma [3]. Venous thromboembolism is less frequent in Asian patients with ductal pancreatic adenocarcinoma [4]. The genetic and/or epigenetic significance of this finding is currently unknown. As thromboprophylaxis carries a bleeding risk, biomarkers and score predictors were investigated in order to better select the patients who would benefit from prophylactic anticoagulation [5]. Leukocytosis, neutrophilia, monocytosis and thrombocytosis, but not lymphocytosis are all risk factors for thromboembolism in cancer patients [6, 7]. Persistent leukocytosis after first cycle of chemotherapy imparts a 3% risk for venous thromboembolism, as opposed to 1.2% for normal leukocyte counts [8]. Moreover, thrombocytosis is associated with a 2.5 fold risk of venous thromboembolism [9]. A hemoglobin level lower than 10 g/dL and/or the use of erythropoiesis-stimulating agents (ESAs) confer a 1.8- fold increased risk of developing VTE [6]. Contrary to early reports, microparticle-associated tissue factor activity does not appear to play an essential role in the prothrombotic state associated with metastatic pancreatic cancer [10, 11]. Nevertheless, its activity is increased and its small effect in fibrin formation may be part of the multifactorial pathogenesis of venous thromboembolism in the adenocarcinoma of the pancreas [10]. Low-dose warfarin and LMWH are safe for prophylactic anticoagulation in pancreatic cancer [12-14]. Table 1 shows the Khorana and Vienna assessment scores for prediction of venous thromboembolism.
What Did We Learn at 2014 ASCO Annual Meeting?
The Impact of Prothrombotic Mutations, PSGL-1 VNTR Polymorphism, Tissue Factor, and Soluble P-Selectin on Venous Thromboembolism in Cancer Patients with Adenocarcinoma
Bozkurt et al. evaluated the frequency of inherited (Factor V of Leiden, prothrombin G20210A mutations and PSGL-1 VNRT polymorphisms) and carcinogenesisacquired (Tissue Factor and soluble P-Selectin) protein genotypes and levels respectively in a patients with adenocarcinoma [15]. From a screened population of 1,838 patients with adenocarcinoma, 63 patients with venous thromboembolism and 38 controls had their blood tested for the above mutations and levels. In the population with venous thromboembolism, tissue factor levels were higher in patients with pancreatic adenocarcinoma than those with other tumors (p=0.02). Also, the PSGL-1 VNRT polymorphisms AB and AC were more frequent in central venous catheter related, subclavian, jugular and pelvic venous thromboembolism.
Incidence of Incidental and Symptomatic Venous Thromboembolism (VTE) and Khorana’s Score in Ambulatory Pancreatic Cancer Patients Receiving Chemotherapy
Muñoz Martin et al. designed a multicentric retrospective cross-sectional study involving a population of ambulatory patients with exocrine pancreatic cancer (EPC) treated with chemotherapy, where the investigators followed 517 patients from January 2008 to December 2011 [16]. Venous thromboembolism was identified in 22.6 % of the patient with a median time to diagnosis of 3 months and 67% of cases occurring within 6 months of diagnosis. Around 50% of the patients had incidental venous thromboembolism. Interestingly visceral thromboembolism was an incidental finding in 91% of the identified cases, representing 38% of all cases of venous thromboembolism in the study. The Khorana score consolidated its clinical usefulness when it predicted symptomatic venous thromboembolism while having no predictive value for incidental venous thromboembolism.
Risk Factors for Cancer-Related Venous Thromboembolism in Ambulatory Patients
Cella et al. validated the Khorana score and identified additional predictor factors for venous thromboembolism in their ambulatory oncologic population on antineoplastic therapy [17]. They followed up 544 ambulatory patients with various cancers, 8% of them with pancreatic cancer. Among the confirmed risk factors were previous venous thromboembolism, metastatic disease, vascular or lymphatic compression by the tumor, extremity edema of extremities, surgical procedure in the last 6 months, and central venous catheter. Venous thromboembolism associated with cancer surgery has been increasing frequency although mortality associated with surgery has been decreasing [18]. This new risk factors help to define which population of oncologic patients would benefit most from prophylactic anticoagulation.
Discussion
Venous thromboembolism is a frequent event in ductal adenocarcinoma. Scores carrying predictive value will support the indication of prophylactic anticoagulation for patients at low bleeding risk and high risk for venous thromboembolism. Biomarkers, especially acquired circulating factors and inherited gene polymorphisms, will redefine venous thromboembolism care in the genomic era. It is now known that Asian patients with ductal adenocarcinoma of the pancreas have lower incidence of venous thromboembolism. It remains to be described if this effect is a consequence of genetics or behaviors (i.e. smoking, metabolic syndrome and diet) affecting epigenetic silencing or activation of cancer pathways. The ESA therapy is one of the components of predicting scores and International Guidelines clearly recommend prophylactic anticoagulation for chemotherapy combinations of thalidomide or lenalidomide and steroids; redefining risks for newly developed monoclonal antibodies and combination chemotherapy for pancreatic cancer and confirming in phase III trials the role of anticoagulation in clinical outcomes will further refine the role of prophylactic anticoagulation in ductal adenocarcinoma.
Conflict of Interest
The authors hereby state that there is no conflict of interest to disclose during the time of submission of this manuscript.
References
- Farge D, Debourdeau P, Beckers M, Baglin C, Bauersachs RM, Brenner B, Brilhante D, et al. International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. J ThrombHaemost. 2013; 11(1): 56-70. [PMID:23217107]
- Lyman GH, Eckert L, Wang Y, Wang H, Cohen A. Venous thromboembolism risk in patients with cancer receiving chemotherapy: a real-world analysis. Oncologist. 2013; 18(12): 1321-9. [PMID:24212499]
- Pabinger I, Ay C. Risk of venous thromboembolism and primary prophylaxis in cancer. Should all patients receive thromboprophylaxis? Hamostaseologie. 2012; 32(2): 132-137. [PMID:21822526]
- Habib M, Saif MW. Thromboembolism and anticoagulation in pancreatic cancer. JOP. 2013; 14(2): 135-7. [PMID:23474555]
- Pabinger I, Thaler J, Ay C. Biomarkers for prediction of venous thromboembolism in cancer. Blood. 2013; 122(12): 2011-8. [PMID:23908470]
- Khorana AA, Francis CW, Culakova E, Lyman GH. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer. 2005; 104(12): 2822-2829. [PMID:16284987]
- Connolly GC, Khorana AA, Kuderer NM, Culakova E, Francis CW, Lyman GH. Leukocytosis, thrombosis and early mortality in cancer patients initiating chemotherapy. Thromb Res. 2010; 126(2): 113-118.
- Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008; 111(10): 4902-4907. [PMID:18216292]
- Zakai NA, Wright J, Cushman M. Risk factors for venous thrombosis in medical inpatients: validation of a thrombosis risk score. J ThrombHaemost. 2004; 2(12): 2156-2161. [PMID:15613021]
- Thaler J, Koder S, Kornek G, Pabinger I, Ay C. Microparticle-associated tissue factor activity in patients with metastatic pancreatic cancer and its effect on fibrin clot formation. Transl Res. 2014; 163(2): 145-50. [PMID:23973167]
- Geddings JE, Mackman N. Tumor-derived tissue factor-positive microparticles and venous thrombosis in cancer patients. Blood. 2013; 122(11): 1873-80. [PMID:23798713]
- Pelzer U, Hilbig A, Stieler JM, Bahra M, Sinn M, Gebauer B, Dörken B, RiessH. Intensified chemotherapy and simultaneous treatment with heparin in outpatients with pancreatic cancer - the CONKO 004 pilot trial. BMC Cancer. 2014; 14: 204. [PMID:24641937]
- Nakchbandi W, et al. Prospective study on warfarin and regional chemotherapy in patients with pancreatic carcinoma. J Gastrointestin Liver Dis. 2008; 17(3): 285-90. [PMID:18836621]
- Icli F, Akbulut H, Utkan G, Yalcin B, Dincol D, Isikdogan A, Demirkazik A, et al. Low molecular weight heparin (LMWH) increases the efficacy of cisplatinum plus gemcitabine combination in advanced pancreatic cancer. J SurgOncol. 2007; 95(6): 507-12. [PMID:17192920]
- Bozkurt M, Okutur K, Aydin K, et al. The impact of prothrombotic mutations, PSGL-1 VNTR polymorphism, tissue factor, and soluble P-selectin on venous thromboembolism in cancer patients with adenocarcinoma. J ClinOncol 32, 2014 (suppl; abstr e22049)
- Muñoz Martin AJ, Adrian SG, Luisa Sánchez Lorenzo LS, et al. Incidence of incidental and symptomatic venous thromboembolism (VTE) and Khorana’s score in ambulatory pancreatic cancer patients receiving chemotherapy. ClinOncol 32, 2014 (suppl; Abstract #e15187) Trinh VQ, Karakiewicz PI, Sammon J, Sun M, Sukumar S, Gervais MK, Shariat SF, et al. Venous thromboembolism after major cancer surgery: temporal trends and patterns of care. JAMA Surg. 2014; 149(1): 43-9. [PMID:24197279]
- Trinh VQ, Karakiewicz PI, Sammon J, Sun M, Sukumar S, Gervais MK, Shariat SF, et al. Venous thromboembolism after major cancer surgery: temporal trends and patterns of care. JAMA Surg. 2014; 149(1): 43-9. [PMID:24197279]

