Case Blog - (2016) Volume 2, Issue 2
Total Kissing Balloon: A Novel Technique to Treat Aneurysmal Left Main Coronary Artery
Alfonso Jurado-Román*, Andrea Moreno-Arciniegas, Ignacio Sánchez-Pérez, María T López-Lluva, Jesús Piqueras-Flores and Fernando Lozano-Ruíz-Poveda
Interventional Cardiology Department, University General Hospital of Ciudad Real, Ciudad Real, Spain
*Corresponding Author:
Alfonso Jurado-Román
Interventional Cardiology Department, University General Hospital of Ciudad Real, Ciudad Real, Spain
Tel: 0034629871863
E-mail: alfonsojuradoroman@gmail.com
Received date: August 01, 2016; Accepted date: August 28, 2016; Published date: August 30, 2016
Citation: Jurado-Román A, Moreno-Arciniegas A, Sánchez-Pérez I, et al. Total Kissing Balloon: A Novel Technique to Treat Aneurysmal Left Main Coronary Artery. Interv Cardiol J 2016, 2:2.
Abstract
An 84 years-old male was admitted for stable angina and an early positive treadmill test. He presented an angiographic severe ostial stenosis of the left main (LM) with no other significant lesions. Intravascular ultrasound image (IVUS) showed a fibro-calcified plaque with a minimal luminal area (MLA) of 3.9 mm2 (Figure1A-asterisk) and a reference diameter of 5.8 mm. A percutaneous coronary intervention (PCI) was scheduled the following day.
Case Blog
An 84 years-old male was admitted for stable angina and an early positive treadmill test.
He presented an angiographic severe ostial stenosis of the left main (LM) with no other significant lesions. Intravascular ultrasound image (IVUS) showed a fibro-calcified plaque with a minimal luminal area (MLA) of 3.9 mm2 (Figure1A-asterisk) and a reference diameter of 5.8 mm. A percutaneous coronary intervention (PCI) was scheduled the following day.
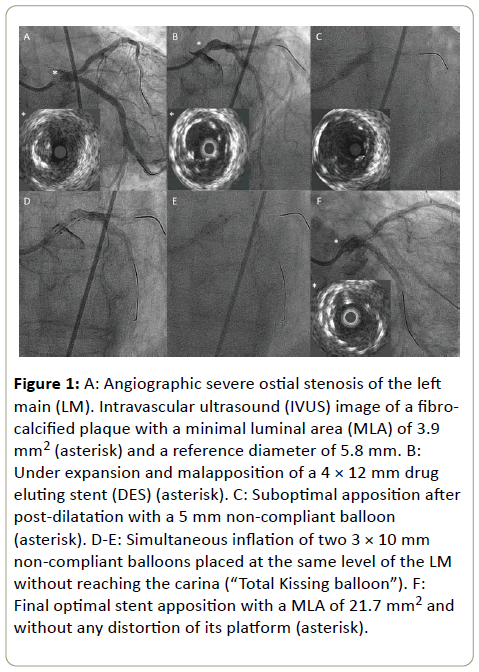
Figure 1: A: Angiographic severe ostial stenosis of the left main (LM). Intravascular ultrasound (IVUS) image of a fibrocalcified plaque with a minimal luminal area (MLA) of 3.9 mm2 (asterisk) and a reference diameter of 5.8 mm. B: Under expansion and malapposition of a 4 × 12 mm drug eluting stent (DES) (asterisk). C: Suboptimal apposition after post-dilatation with a 5 mm non-compliant balloon (asterisk). D-E: Simultaneous inflation of two 3 × 10 mm non-compliant balloons placed at the same level of the LM without reaching the carina (“Total Kissing balloon”). F: Final optimal stent apposition with a MLA of 21.7 mm2 and without any distortion of its platform (asterisk).
However, several hours later the patient presented intractable angina with diffuse ST depression and hemodynamic instability with severe hypotension that needed intravenous inotropic drugs. Thus, an emergent PCI was performed. Predilatation with a 4 × 8 mm balloon was performed and, due to the unavailability of a larger diameter drug eluting stent (DES), a 4 × 12 mm DES was implanted at ostial LM.
Under expansion and malapposition were observed so post dilatation with the largest available diameter balloon (5 mm) was performed. Although improved, no optimal apposition was achieved, so we performed a simultaneous inflation of two 3 × 10 mm non-compliant balloons placed at the same level of the LM without reaching the carina (“Total Kissing balloon”) obtaining optimal stent apposition with a MLA of 21.7 mm2 and without any distortion of its platform (Figure 1).
Large size LM PCI may be challenging due to the absence of DES or balloons that are large enough to reach the reference diameter of the vessel. Simultaneous inflation of two balloons contacting between themselves in their entire length and without involving a bifurcation is a variant of the kissingballoon technique [1]. This "Total Kissing-Balloon" technique, which to our knowledge has not been described in this setting, could be useful in this scenario.
References
- George BS, Myler RK, Stertzer SH, Clark DA, Cote G, et al. (1986) Balloon angioplasty of coronary bifurcation lesions: the kissing balloon technique. Cathet Cardiovasc Diagn 12: 124-138.

