Keywords
Biliary Fistula; Duodenum; Pancreas; Pancreatic Fistula; Pancreaticoduodenectomy; Wounds and Injuries
INTRODUCTION
Pancreaticoduodenal injuries are often associated with complicated treatment strategies [1, 2]. Severe pancreaticoduodenal injuries involve a significant mortality rate ranging from 10 to 36% [3, 4, 5]. The extent of the pancreatic injury is not often evident on an initial computed tomography scan [6]. A variety of approaches to pancreatic trauma have been reported [1, 6, 7]. Pancreaticoduodenectomy for combined pancreaticoduodenal injuries is rarely resorted to in the trauma setting owing to severe concomitant injuries [3, 4, 8, 9]. Moreover, the release of pancreatic enzymes and bile may jeopardize anastomosis [7, 10]. In a series of 48 patients with pancreatic trauma, a pancreaticoduodenectomy was performed in only two patients [7]. Asensio et al. [5] reported a 5% incidence of pancreaticoduodenectomy for patients with pancreatic and duodenal injuries. Pancreaticoduodenectomy should be reserved for patients who have a devascularized pancreatic head or when the ampulla is damaged [4, 9, 11, 12]. The philosophy of the management of complex pancreaticoduodenal injuries is to avoid complex reconstructive procedures in an unstable patient [13]. The use of an abbreviated laparotomy may be helpful in salvaging moribund patients having combined pancreaticoduodenal injuries [4, 10]. Drainage with the formation of a controlled pancreatic fistula carries a low mortality rate, has acceptable morbidity and should be preferred over a pancreaticoenteric anastomosis [14]. Reconstruction can be carried out subsequently [4, 15]. The principle of a staged laparotomy applied to pancreaticoduodenal injuries could lead to improved survival in these patients [4, 10, 13].
The objective of this study was to review our experience with a staged approach (delayed reconstruction) for complex pancreaticoduodenal injuries.
PATIENTS AND METHODS
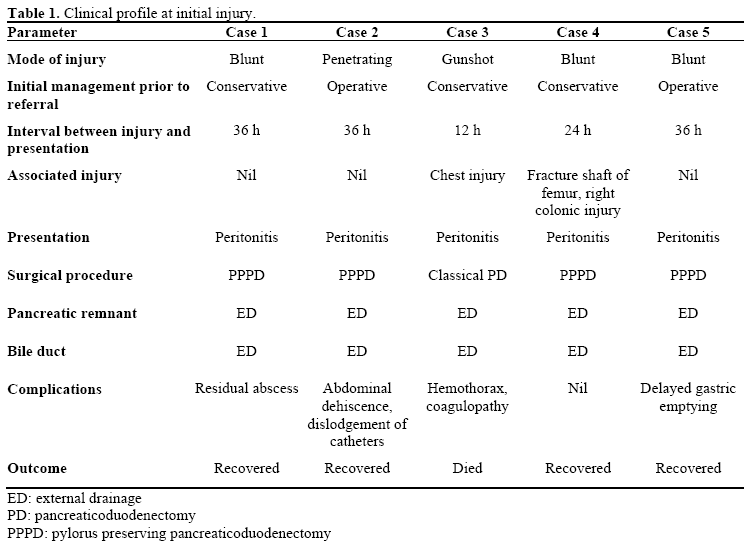
The records of five patients with complex pancreaticoduodenal injuries were reviewed over a period of five years, from March 2003 to March 2008. The mode of injury was blunt trauma in three, and penetrating in two (one stab wound and one gunshot wound). All patients were male, and their ages ranged from 17 to 34 years. All patients had peritonitis at presentation and underwent an urgent operative exploration. Two patients were operated on at another hospital and had a bile drainage tube in place before being transferred to our hospital for specialized care. No imaging studies were undertaken as all the patients were acutely ill at presentation. Two patients had associated injuries: a fracture shaft femur in one and hemopneumothorax requiring chest tube insertion in the other (Table 1).
Operative Findings
Two patients had pancreaticoduodenal disconnection with ampullary disruption, two had extensive laceration of the medial wall of the duodenum with laceration of the pancreatic head, and one had devascularization of the duodenum and a devitalized head of the pancreas. Pancreaticoduodenectomy was performed in these patients: four patients underwent a pylorus-preserving pancreaticoduodenal resection and a classical Whipple procedure was carried out in one owing to the extensive damage to the antrum.
The common bile duct was transected as low as possible to preserve its length. The lower end was closed with absorbable sutures and a T-tube was placed through a choledochotomy. The pancreas was soft with evidence of localized pancreatitis. No attempt was made to completely remove the uncinate process. The pancreatic duct was identified and drained externally with a 6 F infant feeding tube/umbilical vein cannula. Gastrointestinal continuity was restored. A feeding jejunostomy tube was placed in all cases, 20 cm distal to the gastroenteric anastomosis to provide postoperative nutritional support (Figure 1). A large bore (32 F) tube drain was placed close to the pancreatic bed in the right upper abdomen to allow the egress of any residual infection.
Figure 1. Line diagram to demonstrate the method of
biliary and pancreatic exteriorization. A T-tube has
been placed in the bile duct. Note the division of the
bile duct below the level of the cystic duct. The
pancreatic remnant has been exteriorized with a tube in
the pancreatic duct. The enteric continuity has been
restored. A feeding tube has been placed.
Postoperaive Course
One patient died in the immediate postoperative period due to coagulopathy. Post-operative complications were intraabdominal abscess in one requiring imageguided drainage, delayed gastric emptying in one, and abdominal wound dehiscence and dislodgement of drainage tubes in one (Table 1). None of these patients needed surgical intervention. Their hospital stay ranged from 14 to 42 days.
Delayed Reconstruction
Reconstruction was undertaken from 6 to 28 weeks later in four patients. CECT performed prior to the reconstruction showed a normal pancreas and decompressed biliary system (Figure 2). In an isolated Roux loop of the jejunum, a pancreaticojejunostomy and a hepaticojejunostomy were performed in three patients. In one patient, only a hepaticojejunostomy could be performed as there were dense adhesions in the region of the pancreas. The postoperative course was uneventful.
Figure 2. CECT performed prior to reconstruction
shows a normal pancreas. The pancreatic catheter
(arrow) can be seen in situ. Note the biliary system is
decompressed.
Follow-up
The follow-up period ranged from 6 to 24 months. All the patients are well on followup.
DISCUSSION
The surgical management of combined pancreaticoduodenal injuries is complex and the options vary from repair and external drainage to pancreaticoduodenectomy [1, 12, 16]. Pancreaticoduodenectomy is reserved for patients with uncontrollable bleeding from the pancreatic head, proximal pancreatic duct or ampullary injuries which preclude reconstruction, and extensive devitalization of the duodenum and pancreatic head.
We had to resort to a Whipple procedure in all our patients because of devastating injury and uncontrolled bleeding. Leaving behind devitalized tissue would have resulted in postoperative bleeding and infective complications. Pancreaticoduodenectomy in our patients was essentially a debridement procedure to salvage these critically ill patients. Controlled external drainage of the bile and pancreatic ducts facilitates postoperative care and prevents on-going contamination of the peritoneal cavity. The technique of external drainage as an alternative to pancreatic enteric anastomosis is safe and simple to perform, and no complications of the external drainage of the pancreatic duct have been reported [17].
In a relatively stable patient, pancreaticoduodenectomy with or without reconstruction may be a valid option [12, 18]. The mortality rate of a pancreaticoduodenectomy in an emergency situation is high [3, 19]. In one series, the mortality rate of acute pancreaticoduodenectomy exceeded 30% [9]. The main factor responsible for these high morbidity and mortality rates in pancreatic injury is an elevated pancreas-associated complication rate [7, 9, 20]. The factors responsible for an anastomotic leak are associated pancreatitis, a soft and friable pancreas and an undilated normal sized pancreatic duct. A variety of procedures have been advocated to minimize the anastomotic leak rate but no one of these has shown a clear advantage over the other [21]. Moreover, their application in an emergency situation is not well established. Chances of a pancreatic leak are high while working in the presence of a normal, soft pancreas. A controlled external fistula is safe. The vast majority of pancreatic leaks resolve spontaneously with control of sepsis and adequate drainage [22, 23]. Spontaneous healing of a pancreatic leak has been described [24]. Spontaneous healing of a fistula occurred in one patient and the patient is well on follow-up. In view of this high mortality rate, it is debatable whether a pancreaticoduodenectomy should be carried out on an emergency basis; there is a need to adopt a bailout procedure in these complex injuries [10, 25]. A damage control procedure in unstable patients in the form of externally draining the pancreas and biliary tree could be a lifesaving approach [25, 26, 27].
A staged procedure has been advocated in this difficult situation [5, 15, 27, 28]. This entails pancreaticoduodenal resection and biliopancreatic exteriorization as a damage control measure [14]. The stomach, jejunum and pancreatic stump are stapled off. The common bile duct is ligated or drained, the gallbladder is not removed and may be used for biliaryenteric reconstruction. It is not necessary to remove the uncinate process. This simplifies the procedure as the surgeon can operate away from the superior mesenteric vein [29]. One of the most time consuming and demanding steps during pancreaticoduodenectomy is the dissection of the uncinate process which can result in severe intra-operative bleeding and is a difficult and frustrating experience. Leaving behind the uncinate process shortens the operating time with less blood loss. The application of endovascular clips has also been advocated to deal with the uncinate process [30] but may not be applicable in the setting of trauma, especially in an unstable patient. Pancreatic duct ligation has been advocated as an option in unstable patients and when faced with a soft normal pancreas [31]. A low output pancreatic leak resolves spontaneously [23, 24].
Reconstruction is delayed to allow intraabdominal sepsis to be resolved. Following reconstruction, none of the patients in our series developed a pancreatic anastomotic leak. This was due to the firm texture of the pancreas which holds sutures well.
There is a paucity of published studies attesting to the usefulness of delayed reconstruction in complex pancreaticoduodenal injuries [5, 15, 16, 27, 32]. Our results have shown the usefulness of a staged pancreaticoduodenectomy as a damage control measure and a delayed reconstruction in these critically ill patients. Four of the five patients survived. The management of severe pancreaticoduodenal injuries is one of the most difficult challenges. Initial damage control and the application of delayed reconstruction may be an optimal choice in that they can obviate complications such as anastomotic breakdown.
Conflict of interest
The authors have no potential conflicts of interest
References
- Degiannis E, Glapa M, Loukogeorgakis SP, Smith MD. Management of pancreatic trauma. Injury 2008; 39:21-9. [PMID 17996869]
- Krige JE, Beningfield SJ, Nicol AJ, Navsaria P. The management of complex pancreatic injuries. S Afr J Surg 2005; 43:92-102. [PMID 16180395]
- Vasquez JC, Coimbra R, Hoyt DB, Fortlage D. Management of penetrating pancreatic trauma: an 11- year experience of a level-1 trauma center. Injury 2001; 32:753-9. [PMID 11754881]
- Lopez PP, Benjamin R, Cockburn M, Amortegui JD, Schulman CI, Soffer D, et al. Recent trends in the management of combined pancreatoduodenal injuries. Am Surg 2005; 71:847-52. [PMID 16468533]
- Asensio JA, Petrone P, Roldán G, Kuncir E, Demetriades D. Pancreaticoduodenectomy : a rare procedure for the management of complex pancreaticoduodenal injuries. J Am Coll Surg 2003; 197:937-42. [PMID 14644281]
- Vane DW, Klankhooy A, Sartorelli KH, Vane JL. Initial resection of potentially viable tissue is not optimal treatment for grade II - IV pancreatic injuries. World J Surg. 2008 Apr 11. [Epub ahead of print] [PMID 18404287]
- Lin BC, Chen RJ, Fang JF, Hsu YP, Kao YC, Kao JL. Management of blunt major pancreatic injury. J Trauma 2004; 56:774-8. [PMID 15187740]
- Olah A, Issekutz A, Manlik L, Makay R. Pancreatic transection from blunt abdominal trauma: early versus delayed diagnosis and surgical management. Dig Surg 2003; 20: 408-14. [PMID 12900531]
- Feliciano DV, Martin TD, Cruse PA, Graham JM, Burch JM, Mattox KL, et al. Management of combined pancreaticoduodenal injuries. Ann Surg 1987; 205:673- 80. [PMID 3592810]
- Wang GF, Li YS, Li JS. Damage control surgery for severe pancreatic trauma. Hepatobiliary Pancreat Dis Int 2007; 6:569-71. [PMID 18086619]
- Phelan HA, Minei JP. Pancreatic trauma: diagnostic and therapeutic strategies. Curr Treat Options Gastroenterol 2005; 8:355-63. [PMID 16162301]
- DeKerpel W, Hendrickx T, Vanrykel J-P, Aelvoet C, DeWeer F. Whipple procedure after blunt abdominal trauma. J Trauma 2002; 53:780-3. [PMID 12394884]
- Rickard MJ, Brohi K, Bautz PC. Pancreatic and duodenal injuries: keep it simple. Anz J Surg 2005; 75:581-6. [PMID 15972052]
- Degiannis E, Levy RD, Velmahos GC, Potokar T, Florizone MG, Saadia R. Gunshot injuries of the head of the pancreas: conservative approach. World J Surg 1996; 20:68-71. [PMID 8588416]
- Koniaris LG, Mandal AK, Genuit T, Cameron JL. Two-stage trauma pancreaticoduodenectomy: delay facilitates anastomotic reconstruction. J Gastrointest Surg 2000; 4:366-9. [PMID 11058854]
- Krige JE, Nicol AJ, Navsaria PH, Jones O, Bornman PC. Emergency pancreaticoduodenectomy for complex pancreatic trauma. HPB Surg 2005; 7:104.
- Katsaragakis S, Antonakis P, Konstadoulakis MM, Androulakis G. Reconstruction of the pancreatic duct after pancreaticoduodenectomy: a modification of the Whipple procedure. J Surg Oncol 2001; 77: 26-9. [PMID 11344478]
- Eastlick L, Fogler RJ, Shaftan GW. Pancreaticoduodenectomy for trauma : delayed reconstruction : a case report. J Trauma 1990; 30:503- 5. [PMID 2325184]
- Chrysos E, Arthanasakis E, Xynos E. Pancreatic trauma in the adult: current knowledge in diagnosis and management. Pancreatology 2002; 2: 365-78. [PMID 12138225]
- Mayer JM, Tomczak R, Rau B, Gebhard F, Beger HG. Pancreatic injury in severe trauma: early diagnosis and therapy improve the outcome. Dig Surg 2002; 19:291-7. [PMID 12207073]
- Fisher WE, Chai C, Hodges SE, Wu M-F, Hilsenbeck SG, Brunicardi FC. Effect of bioglue on the incidence of pancreatic fistula following pancreas resection. J Gastrointest Surg 2008; 12:882-90. [PMID 18273671]
- Beecherl EE, Shires GT, Shires GT. Treatment of post-pancreaticoduodenectomy complications. Curr Treat Options Gastroenterol 2004; 7:365-70. [PMID 15345207]
- Leppanienii A. Management of pancreatic and duodenal injuries. Lithuanian Surgery 2007; 5:102-7.
- Chirletti P, Caronna R, Cardi M, Pittau G, Schiratti M, Romeo G, Tarantino E, et al. Reconstruction after pancreaticoduodenectomy with a double jejunal loop: advantages and technical aspect of a personal technique. JOP. J Pancreas (Online) 2006; 7(Suppl 5):559. [PMID 17003523]
- el-Boghdadly S, al-Yousef Z, al Bedah K. Pancreatic injury: an audit and a practical approach. Ann R Coll Surg Engl 2000; 82:258-62. [PMID 10932660]
- Schoretsanitis GN, Tsiftsis DD, Tatoulis PA, Gontikakis ET. Pancreaticoduodenectomy with external drainage of residual pancreatic duct. Eur J Surg 1993; 159:421-4. [PMID 8105978]
- Tuech JJ, Pessaux P, Rege N, Bergamaschi R, Arnaud JP. Emergency Pancreaticoduodenectomy with Delayed Reconstruction for Bleeding: A Life Saving Procedure. Int J Gastrointest Cancer 2001; 29:59-62. [PMID 12754406]
- Koniaris LG. Role of pancreatectomy after severe pancreaticoduodenal trauma. J Am Coll Surg 2004; 198:677-8. [PMID 15051028]
- Hirshberg A, Mattox KL. Top knife: the art and craft of trauma surgery. In: The wounded surgical soul. Shrewsbury, UK: TSM publishing; 2005.
- Kleeff J, Friess H, Buchler MW. Dissection of uncinate process and pancreatic head behind the portal vein using endovascular clips. J Hepatobiliary Pancreat Surg 2007; 14:480-3. [PMID 17909717]
- Gentilello LM, Cortes V, Buechter KJ, Gomez GA, Castro M, Zeppa R. Whipple procedure for trauma: is duct ligation a safe alternative to pancreaticojejunostomy? J Trauma 1991; 31:661-7. [PMID 2030513]
- Kobayashi A, Takagi S, Miwa S, Miyagawa S. Successful treatment for combined pancreatoduodenal injury by a second-stage pancreatojejunostomy following pancreatoduodenectomy. Hepatogastroenterology 2004; 51:1674-5. [PMID 15532802]



