Hassan Aboumerhi1,3, Chad Shultz2 and SA Erzurum1,2,3
1Northeast Ohio Medical University, Rootstown, OH, 44272
2Eye Care Associates, Inc, Poland, OH, 44514
3St Elizabeth Health Center, Youngstown, OH 44501
*Corresponding Author:
Hassan Aboumerhi MD
St. Elizabeth Health Center, 1044 Belmont Ave, Youngstown, OH 44504
Tel: 440.292.7602
E-mail: haboumerhi@neomed.edu
Received Date: November 16, 2015; Accepted Date: December 04, 2015; Published Date: December 08, 2015
Citation: Aboumerhi H,Shult C, Erzurum SA (2016) Traumatic Epithelial Ingrowth Despite Non-Displaced Lasik Flap. J Eye Cataract Surg 1:5. doi: 10.21767/2471-8300.100005
Copyright: © 2016 Aboumerhi H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
LASIK; Epithelial ingrowth; Laser assisted in-situ keratomileusis
Abbreviations
LASIK: Laser Assisted In-situ Keratomileusis; UCVA: Uncorrected Visual Acuity; DLK: Diffuse Lamellar Keratitis; OCT: Optical Coherence Tomography
Introduction
Most patients undergoing laser in situ keratomileusis (LASIK) recover without issue. In certain cases, however, postoperative complications may threaten vision unless treated properly. One of these complications, corneal epithelial ingrowth, often occurs in the first day of 1-2% of LASIK cases [1]. Epithelial cell growth may encroach on the visual axis, impairing vision. These patients may develop corneal melt leading to permanent vision loss if not treated appropriately [2].
The formation of a corneal flap by LASIK leaves a potential space between the flap and the stroma. Etiologies for epithelial ingrowth are twofold: [1] cellular replication after introduction to the interface of the flap from the corneal periphery via cutting, lifting, or flap manipulation and [2] cellular migration from the flap border after surgery [3]. Risk factors for epithelial ingrowth include multiple LASIK procedures and hyperopic correction as opposed to myopic correction [4]. Case reports of traumatic incidents that have disrupted the corneal flap have also been reported, inducing epithelial ingrowth and, in one case, ingrowth was delayed 14 years after initial LASIK [5]. There are no reports of epithelial ingrowth after LASIK without corneal flap displacement. We report a case of epithelial ingrowth after minor corneal abrasion without manipulation or displacement of the LASIK flap 15 years after surgery.
Case Background
A 50-year-old woman with a history of LASIK 15 years ago presented to the emergency room after poking her eye with a twig in her garden. Physical exam demonstrated a corneal abrasion of the left eye. The patient was asked to follow up with her ophthalmologist the next morning. Ophthalmology evaluation demonstrated an uncorrected visual acuity (UCVA) of 20/20 in the right eye. The affected left eye was 20/40, improving to 20/25 on pinhole. The conjunctiva was mildly injected. Slit lamp examination revealed a corneal abrasion of the epithelium temporally at 3 o'clock surrounded by mild corneal edema. The flap was intact, in place, and its edges were uninvolved. The rest of the eye exam was unremarkable. The patient was started on tobramycin/dexmathesaone ophthalmic drops and was asked to return in 1 week.
During the patient's next visit, she described no discomfort and reported vision improvement and symptom resolution. She displayed UCVA of 20/20 in the right eye and 20/25- in the left eye. On slit lamp examination, her left eye exhibited resolution of the corneal abrasion and edema. There was, however, corneal haze noted in the interface directly under the area of the injury that extended toward the visual axis. The flap was still intact. Because of concern for disseminated lamellar keratitis (DLK), prednisolone acetate ophthalmic drops were prescribed for every two hours and the patient was referred to a refractive surgeon.
Five days later, UCVA was 20/20 in her left eye. Slit lamp examination demonstrated moderate epithelial ingrowth under the midperiphery of the flap with direct extension towards the visual axis, preserving a clear zone of interface temporally toward the edge of the flap (Figure 1).
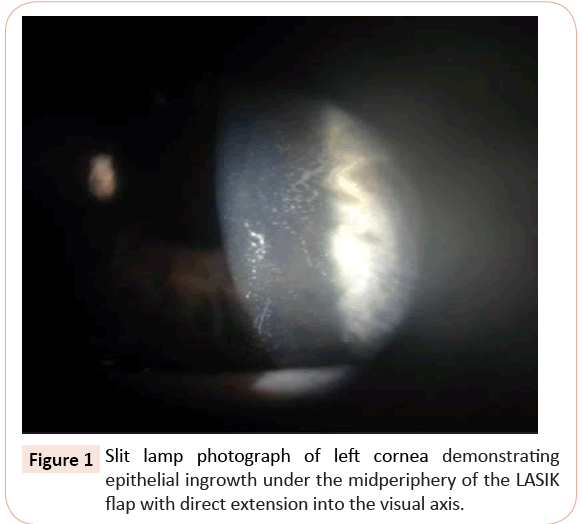
Figure 1: Slit lamp photograph of left cornea demonstrating epithelial ingrowth under the midperiphery of the LASIK flap with direct extension into the visual axis.
Because of significant epithelial organization and imposing threat to the visual axis, the ingrowth was surgically removed. After procedural consent, the flap was lifted after marking the forward edge with a pen. The ingrowth, which extended to the temporal edge of the visual axis, was then peeled away in one piece. After irrigation and careful inspection, the flap was then replaced (Figure 2).
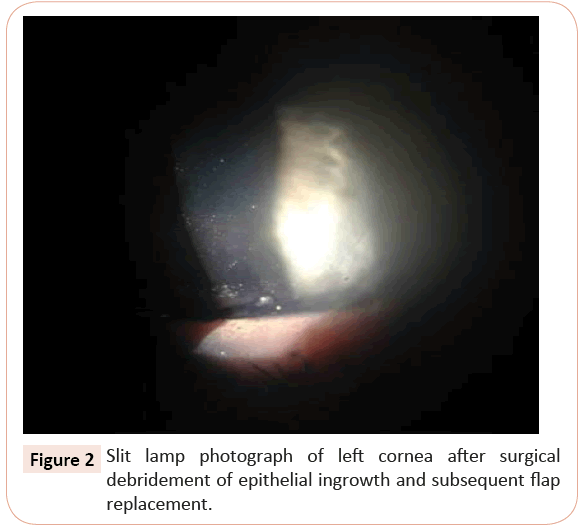
Figure 2: Slit lamp photograph of left cornea after surgical debridement of epithelial ingrowth and subsequent flap replacement.
The patient was prescribed ofloxacin and prednisolone acetate drops and was instructed to return for reevaluation in one day. She returned with a clear visual axis and a smooth flap. One month later, there was no return of epithelial ingrowth and the patient's vision was still 20/20 in both eyes.
Discussion
LASIK permanently changes the inherent anatomy of the cornea. Once a patient undergoes LASIK surgery, the cornea heals exclusively at the periphery of the microkeratome wound away from the visual axis, thereby leaving a persistent potential space under the flap. Even years after LASIK, only minimal adhesions may hold the flap to the stroma/strong>, leaving the rest of the interface patent and predisposing the flap to displacement after trauma [6].
Table 1 describes reported cases of traumatic LASIK flap epithelial ingrowth. Mean patient age was 36 and the female to male ratio was 1:0.67. Five cases in the series were caused by finger sticks to the eye and three were from a twig or branch. Seventy percent experienced full recovery of their vision; thirty percent of patients' visual deficits remained, despite improvement. Two cases did not require debridement of epithelial ingrowth; one case in the series involving corneal perforation mandated penetrating keratoplasty. Our case is the latest-onset of traumatic epithelial ingrowth, 15 years after initial LASIK, and the only case without flap displacement [5-19,20].
| Cases of Traumatic LASIK Flap Epithelial Ingrowth |
| Author |
Year Published |
Patient Age |
Sex |
Time after LASIK |
Eye |
Etiology |
Flap Displacement |
VA, Before |
Treatment |
VA,
After |
| Lemley |
2000 |
37 Yo |
F |
17 m |
OS |
Airbag |
Yes |
20/100 |
Debridement |
20/20 |
| Leung |
2000 |
50Yo |
F |
1 y |
OS |
Bird beak |
Yes |
20/400 |
Debridement |
20/30 |
| Melki |
2000 |
28Yo |
M |
10d |
OS |
Basketball |
Yes |
|
Flap Replacement |
20/30 |
| Melki |
2000 |
21Yo |
M |
24d |
OD |
Fingernail |
Yes |
4/200 |
Debridement |
20/20 |
| Aldave |
2001 |
29Yo |
M |
18m |
OD |
Fingernail |
Yes |
20/200 |
Debridement |
20/40 |
| Patel |
2001 |
28Yo |
F |
10m |
OS |
Fingernail |
Yes |
20/200 |
Debridement |
20/40 |
| Sun |
2001 |
26Yo |
M |
10m |
OD |
Stone |
Yes |
|
Penetrating Keratoplasty |
20/20 |
| Mifflin |
2002 |
37Yo |
M |
3 y |
OS |
Tree branch |
Yes |
20/40 |
Debridement |
20/20 |
| Booth |
2003 |
38Yo |
M |
30m |
OS |
Football |
Yes |
20/25 |
Debridement |
20/20 |
| Srinivasan |
2004 |
23Yo |
F |
4y |
OD |
Fingernail |
Yes |
20/400 |
Flap Replacement |
20/20 |
| Cheng |
2006 |
23Yo |
M |
7 y |
OS |
Fingernail |
Yes |
20/70 |
Debridement |
20/20 |
| Cheng |
2006 |
33Yo |
F |
1 y |
OS |
Broom stick |
Yes |
CF |
Debridement |
20/20 |
| Cheng |
2006 |
38Yo |
F |
2 y |
OD |
Folder |
Yes |
|
Debridement |
20/25 |
| Yeh |
2006 |
50Yo |
F |
21m |
OD |
Bush Twig |
Yes |
20/200 |
Debridement |
20/70 |
| Kim |
2010 |
29Yo |
M |
9y |
OS |
Dog paw |
Yes |
CF |
Debridement |
20/25 |
| Moshirfar |
2011 |
48Yo |
F |
7y |
OS |
Iron Cord |
Yes |
20/40 |
Debridement |
20/20 |
| Holt |
2012 |
59Yo |
F |
14y |
OS |
Blunt wooden block |
Yes |
20/30 |
Debridement |
20/20 |
| Lovieno |
2012 |
45Yo |
F |
2y |
OD |
Cupboard door |
Yes |
20/40 |
Debridement |
20/20 |
| Sinha |
2014 |
26Yo |
F |
4y |
OS |
Wooden Splinter |
Yes |
20/60 |
Debridement |
20/20 |
| Aboumerhi |
2015 |
50Yo |
F |
15y |
OS |
Twig |
No |
20/40 |
Debridement |
20/20 |
Table 1: "Cases of Traumatic LASIK Flap Epithelial Ingrowth." This case study is the latest-onset from initial LASIK and the only case without flap displacement.
In the current case, epithelial ingrowth resolved on slit lamp exam after flap lift, debridement, and drop treatment; her initial symptoms of blurry vision did not return. How the epithelial cells were introduced under the corneal flap remains unclear. Traumatic crystalline foreign bodies at the LASIK flap interface without flap displacement has been reported. Choi postulated that a sharp, high velocity, but weak ocular trauma could open the potential stromal space and leave debris without displacing the flap [21]. We speculate a similar mechanism occurred with this patient or that the twig may have microscopically penetrated to the interface, implanting surface epithelial cells into the potential space. Cellular proliferation may have given the patient their presenting symptoms.
Although corneal slit lamp examination is the standard for detecting epithelial ingrowth, anterior segment optical coherence tomography (OCT) may be a useful diagnostic tool. OCT may evaluate corneal structure changes related to disease before surgical debridement. After treatment, careful monitoring with close follow-up in these patients is necessary. Higher rates of recurrence even after surgical debridement have been reported [22].
Post-traumatic pithelial ingrowth introduces cells into the corneal flap interface and corneal disturbance is observed. In this report, however, epithelial ingrowth occurred beneath the flap without any sign of disruption. This report exemplifies the need for close follow-up and examination of all LASIK patients even after minor trauma, since corneal anatomy is indefinitely altered. Ophthalmologists should educate patients on epithelial ingrowth as a post-operative complication and carefully monitor patients for signs, regardless of observed flap disruption or distant chronology from the initial LASIK procedure.
Acknowledgement
This original research is not under consideration elsewhere; authors have no financial disclosures or conflict of interest. All authors have made contributions to this paper for authorship, including design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Authors have had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
References
- Gimbel HV, Penno EE, van Westenbrugge JA, Ferensowicz M, Furlong MT (1998) Incidence and management of intraoperative and early postoperative complications in 1000 consecutive laser in situ keratomileusis cases. Ophthalmology 105:1839-1847.
- Castillo A, Diaz-Valle D, Gutierrez AR, Toledano N, Romero F (1998) Peripheral melt of flap after laser in situ keratomileusis. Journal of Refractive Surgery14:61-63.
- Nicolas M, Abouzeid H, Deprez M, et al. (2012)Epithelial ingrowth cells after LASIK/ALTK (automated lamellar therapeutic keratoplasty): are they corneal epithelial stem cells? British Journal of Ophthalmology 96:1043-1046.
- Mohamed TA, Hoffman RS, Fine IH, Packer M (2011) Post-laser assisted in situ keratomileusis epithelial ingrowth and its relation to pretreatment refractive error. Cornea 30:550-552.
- Holt DG, Sikder S, Mifflin MD (2012) Surgical management of traumatic LASIK flap dislocation with macrostriae and epithelial ingrowth 14 years postoperatively. J Cataract Refract Surg 38: 357-361.
- Sinha R, Shekhar H, Tinwala S, Gangar A, Titiyal JS (2014) Late post-traumatic flap dislocation and macrostriae after laser in situ keratomileusis. Oman J Ophthalmol 7: 25-27.
- Lemley HL, Chodosh J, Wolf TC, Bogie CP, Hawkins TC (2000) Partial dislocation of laser in situ keratomileusis flap by air bag injury. J Refract Surg 16: 373-374.
- Leung ATS, Rao SK, Lam DSC. (2000) "Traumatic partial unfolding of laser in situ keratomileusis flap with severe epithelial ingrowth." J Cataract Refract Surg26:135-139.
- Melki SA, Talamo JH, Demetriades AM, Jabbur NS, Essepian JP, et al. (2000) Late traumatic dislocation of laser in situ keratomileusis corneal flaps. Ophthalmology 107: 2136-2139.
- Aldave AJ, Hollander DA, Abbott RL (2002) Late-onset traumatic flap dislocation and diffuse lamellar inflammation after laser in situ keratomileusis. Cornea 21: 604-607.
- Patel CK, Hanson R, McDonald B, Cox N (2001) Case reports and small case series: late dislocation of a LASIK flap caused by a fingernail. Arch Ophthalmol 119: 447-449.
- Sun CC, Chang SW, Tsai RRF. (2001)"Traumatic Corneal Perforation withEpithelial Ingrowth After Laser In Situ Keratomileusis." Arch Ophthalmol119:907-909.
- Mifflin M, Kim M (2002) "Laser In Situ Keratomileusis Flap Dehiscence 3 Years Postoperatively." J Cataract Refractive Surg 28:733-735.
- Booth MA, Koch DD (2003) Late laser in situ keratomileusis flap dislocation caused by a thrown football. J Cataract Refract Surg 29: 2032-2033.
- Srinivasan M, Prasad S, Prajna NV (2004) "Late dislocation of LASIK flap following fingernail injury." Indian J Ophthalmology 52:327.
- Cheng AC, Rao SK, Leung GY, Young AL, Lam DS (2006) Late traumatic flap dislocations after LASIK. J Refract Surg 22: 500-504.
- Yeh DL, Bushley DM, Kim T (2006) "Treatment of Traumatic LASIK Flap Dislocation and Epithelial Ingrowth with Fibrin Glue." Am J Ophthalmol 141:960-962.
- Kim HJ, Silverman CM (2010) Traumatic dislocation of LASIK flaps 4 and 9 years after surgery. J Refract Surg 26: 447-452.
- Moshirfar M, Anderson E, Taylor N, Hsu M (2011) “Management of a Traumatic Flap Dislocation Seven Years after LASIK.” Case Reports in Ophthalmological Medicine 2011: 514780.
- Iovieno A, Sharma DP, Wilkins MR (2012) OCT visualization of corneal structural changes in traumatic dislocation of LASIK flap. International Ophthalmology 32:459-460.
- Choi JA, Kim M. (2012) "LASIK Interface-Captured Foreign Bodies after Mild Traumatic Corneal Scratch without Flap Displacement." Korean J Ophthalmol 26:222-225.
- Henry CR, Canto AP, Galor A, Vaddavalli PK, Culbertson WW, et al. (2012) Epithelial ingrowth after LASIK: clinical characteristics, risk factors, and visual outcomes in patients requiring flap lift. Journal of Refractive Surgery 28:488-492.

