Keywords
4-amino-5-(4-methylphenyl)-7-(tert-butyl)pyrazolo (3,4-d)pyrimidine; Amylases; Clinical Trials; Controlled Clinical Trial; Drug Toxicity; Lipase; Pancreatitis
INTRODUCTION
In 2007, Badalov et al. [1] revised the data in the literature on drug-induced acute pancreatitis on the basis of a new classification system; they suggested the following classification: Class Ia - drugs having at least one case report with positive rechallenge, excluding all other causes, such as alcohol, hypertriglyceridemia, gallstones and other drugs; Class Ib - those drugs having at least one case report with positive rechallenge in whom other causes, such as alcohol, hypertriglyceridemia, gallstones and other drugs were not ruled out; Class II - those drugs with at least four cases in the literature and consistent latency (75% of cases or more); Class III - drugs with at least two cases in the literature, no consistent latency among cases and no rechallenge and, finally, Class IV - the drugs not fitting into the above-mentioned classes, having a single case report published in the medical literature, without rechallenge.
The advent of new drugs can rapidly increase the number of substances causing acute pancreatitis. One example is the family of the drugs called “tyrosine kinase inhibitors” which are drugs used for gastrointestinal stromal tumors (imatinib and sunitinib), unresectable hepatocellular carcinomas (sorafenib) and advanced renal cell carcinomas (sorafenib and sunitinib). These drugs are capable of inhibiting VEGF receptors 2 and 3, the platelet-derived growth factor receptor, fms-related tyrosine kinase 3 (FLT3), c-Kit and ret proto-oncogene (RET) [2]. In addition, they inhibit the breakpoint cluster region- Abelson proto-oncogene (BCR-ABL) chimeric protein which is thought to play a central role in the pathogenesis of Philadelphia (Ph) chromosomepositive leukemias, notably chronic myeloid leukemia [3]. Imatinib mesylate represented a major therapeutic advance over conventional chronic myeloid leukemia therapy, with more than 90% of patients obtaining complete hematologic response and 70-80% of patients achieving a complete cytogenetic response. Resistance to imatinib represents a clinical challenge and is often the result of point mutations causing a conformation change in BCR-ABL which impairs imatinib binding. Novel targeted agents designed to overcome imatinib resistance include dasatinib, nilotinib, bosutinib and others [4]. One of the adverse effects of all these drugs is the increase in serum amylase and/or lipase levels [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17], sometimes with very high serum activity levels evaluated according to the Common Terminology Criteria for Adverse Events Version 3.0 (Table 1) [18]. The frequency of the increase in amylase and lipase was high in patients treated with sorafenib and was low for those treated with nilotinib. There are several hypotheses regarding the increase of serum pancreatic enzyme activities and they especially regard nilotinib: 1) nilotinib is able to inhibit the nonreceptor tyrosine kinase c-abl with high affinity; other than the kinase domain, the c-abl protein interacts with signaling proteins, nucleo-cytoplasmic shuttling, DNA and actin binding sites, thus integrating information from multiple pathways in various cellular compartments. Therefore, it is possible that c-abl inhibition might interfere with the molecular mechanisms regulating pancreatic cell death, inducing pancreatic damage; 2) nilotinib may also act on unknown intracellular pathways involved in calcium release from the intracellular acinar stores, which regulate exocrine pancreatic secretion, or may promote the accumulation of fatty acid inside the pancreatic acinar cells, which disturbs exocytosis; however, we should also point out that an increase in the serum concentration of pancreatic enzymes may be an expression of pancreatic involvement during the diseases studied or that elevated amylase and/or lipase levels may also be a non-specific phenomenon without any clinical implication.
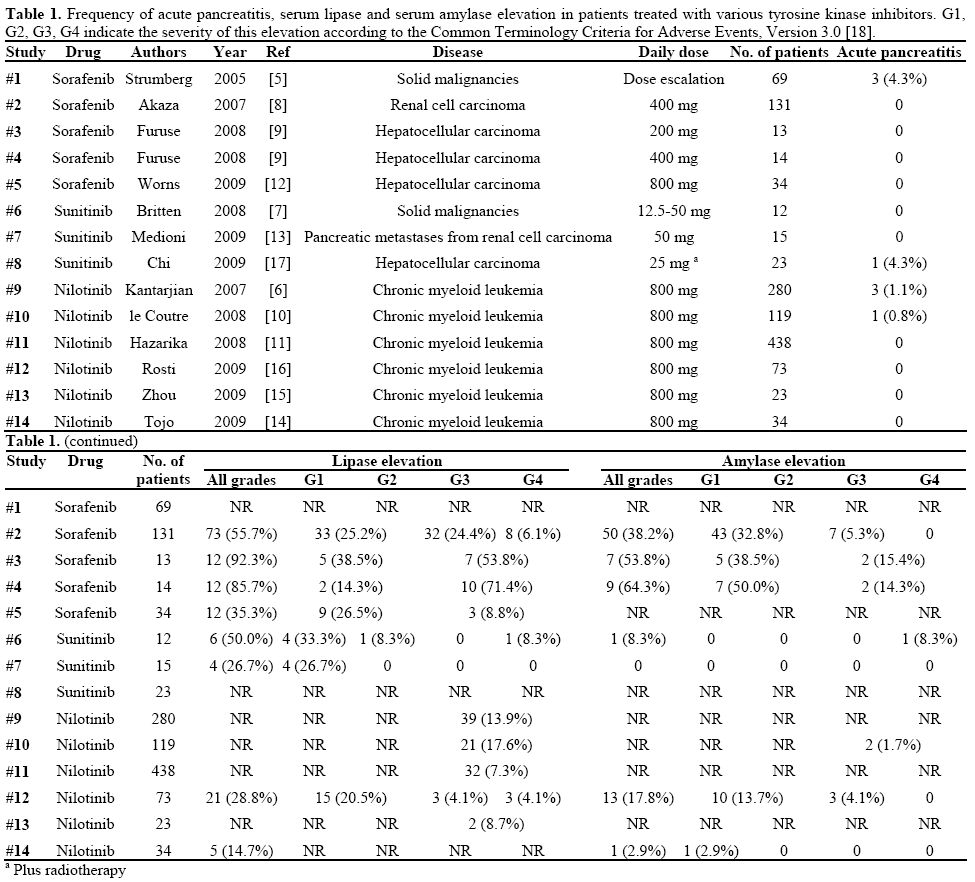
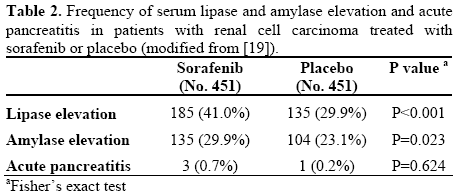
Regarding acute pancreatitis induced by this class of drugs, its frequency is low, ranging from 0 to 4.3% (Table 1). It should be pointed out that all cases of pancreatitis are not fully characterized in the studies in which they have been reported [5, 6, 10, 17] and in these patients we have no information about alcohol habit, the presence of hypertriglyceridemia and the presence of gallstones. In addition, regarding sorafenib alone, it has also been reported that, whereas the drug is capable of significantly increasing serum amylase and lipase activity in renal cell carcinoma patients treated with it in respect to those treated with a placebo, the frequency of acute pancreatitis was not different in patients treated with sorafenib as compared to those treated with a placebo (Table 2) [19]. However, the importance of case reports in the postmarketing surveillance of drugs is central in evaluating the adverse effects of medications; in fact, sorafenib has been implicated as a cause of acute pancreatitis in two cases [20, 21], one of them with positive rechallenge [20]. In this issue of JOP. J Pancreas (Online), the third case of acute pancreatitis induced by sorafenib in a patient with hepatocellular carcinoma has been reported [22]. In all three cases, other causes of acute pancreatitis were ruled out; thus, according to the classification system of Badalov et al. [1], sorafenib can be considered as Class Ia, i.e. a drug with at least one case report with positive rechallenge, excluding all other causes, such as alcohol, hypertriglyceridemia, gallstones and other drugs. The mechanism by which sorafenib induces pancreatitis is unknown; it is probable that the anti-VEGF effects of the drug cause ischemia of the pancreatic tissue, increasing the risk of pancreatitis [23, 24]. It has also been hypothesized that sorafenib may determine gastrointestinal motility abnormalities which in turn may cause alteration of the sphincter of Oddi [20]. However, an individual idiosyncratic effect cannot be ruled out. In conclusion, a new drug, i.e. sorafenib, has been added to the drugs capable of inducing acute pancreatitis and patients should be watched for signs and symptoms of acute pancreatitis. If pancreatitis is suspected, sorafenib and other potentially suspect drugs should be discontinued. Whether acute pancreatitis due to tyrosine kinase inhibitors is associated only with sorafenib or may be also caused by other drugs of the same class, such as sunitinib or nilotinib, remains an open question.
Conflict of Interest The authors have no potential conflict of interest
References
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol 2007; 5:648-61. [PMID 17395548]
- Cabanillas ME, Waguespack SG, Bronstein Y, Williams MD, Feng L, Hernandez M, et al. Treatment with tyrosine kinase inhibitors for patients with differentiated thyroid Cancer: the M. D. Anderson experience. J Clin Endocrinol Metab 2010; Apr 14. [PMID 20392874]
- Deininger MW, Vieira S, Mendiola R, Schultheis B, Goldman JM, Melo JV. BCR-ABL tyrosine kinase activity regulates the expression of multiple genes implicated in the pathogenesis of chronic myeloid leukemia. Cancer Res 2000;60:2049-55. [PMID 10766197]
- Jabbour E, Fava C, Kantarjian H. Advances in the biology and therapy of patients with chronic myeloid leukaemia. Best Pract Res Clin Haematol 2009; 22:395-407. [PMID 19959090]
- Strumberg D, Richly H, Hilger RA, Schleucher N, Korfee S, Tewes M, et al. Phase I clinical and pharmacokinetic study of the Novel Raf kinase and vascular endothelial growth factor receptor inhibitor BAY 43-9006 in patients with advanced refractory solid tumors. J Clin Oncol 2005; 23:965-72. [PMID 15613696]
- Kantarjian H, Giles F, Wunderle L, Bhalla K, O'Brien S, Wassmann B, et al. Nilotinib in imatinib-resistant CML and Philadelphia chromosome-positive ALL. N Engl J Med 2006; 354:2542-51. [PMID 16775235]
- Britten CD, Kabbinavar F, Hecht JR, Bello CL, Li J, Baum C, Slamon D. A phase I and pharmacokinetic study of sunitinib administered daily for 2 weeks, followed by a 1-week off period. Cancer Chemother Pharmacol 2008; 61:515-24. [PMID 17505827]
- Akaza H, Tsukamoto T, Murai M, Nakajima K, Naito S. Phase II study to investigate the efficacy, safety, and pharmacokinetics of sorafenib in Japanese patients with advanced renal cell carcinoma. Jpn J Clin Oncol 2007; 37:755-62. [PMID 17951335]
- Furuse J, Ishii H, Nakachi K, Suzuki E, Shimizu S, Nakajima K. Phase I study of sorafenib in Japanese patients with hepatocellular carcinoma. Cancer Sci 2008; 99:159-65. [PMID 17953709]
- le Coutre P, Ottmann OG, Giles F, Kim DW, Cortes J, Gattermann N, et al. Nilotinib (formerly AMN107), a highly selective BCR-ABL tyrosine kinase inhibitor, is active in patients with imatinib-resistant or -intolerant accelerated-phase chronic myelogenous leukemia. Blood 2008; 111:1834-9. [PMID 18048643]
- Hazarika M, Jiang X, Liu Q, Lee SL, Ramchandani R, Garnett C, et al. Tasigna for chronic and accelerated phase Philadelphia chromosome--positive chronic myelogenous leukemia resistant to or intolerant of imatinib. Clin Cancer Res 2008; 14:5325-31. [PMID 18765523]
- Wörns MA, Weinmann A, Pfingst K, Schulte-Sasse C, Messow CM, Schulze-Bergkamen H, et al. Safety and efficacy of sorafenib in patients with advanced hepatocellular carcinoma in consideration of concomitant stage of liver cirrhosis. J Clin Gastroenterol 2009; 43:489-95. [PMID 19247201]
- Medioni J, Choueiri TK, Zinzindohoué F, Cho D, Fournier L, Oudard S. Response of renal cell carcinoma pancreatic metastasis to sunitinib treatment: a retrospective analysis. J Urol 2009; 181:2470- 5. [PMID 19371877]
- Tojo A, Usuki K, Urabe A, Maeda Y, Kobayashi Y, Jinnai I, et al. A Phase I/II study of nilotinib in Japanese patients with imatinibresistant or -intolerant Ph+ CML or relapsed/refractory Ph+ ALL. Int J Hematol 2009; 89:679-88. [PMID 19449194]
- Zhou L, Meng F, Yin O, Wang J, Wang Y, Wei Y, et al. Nilotinib for imatinib-resistant or -intolerant chronic myeloid leukemia in chronic phase, accelerated phase, or blast crisis: a singleand multiple-dose, open-label pharmacokinetic study in Chinese patients. Clin Ther 2009; 31:1568-75. [PMID 19695406]
- Rosti G, Palandri F, Castagnetti F, Breccia M, Levato L, Gugliotta G, et al. Nilotinib for the frontline treatment of Ph(+) chronic myeloid leukemia. Blood 2009; 114:4933-8. [PMID 19822896]
- Chi KH, Liao CS, Chang CC, Ko HL, Tsang YW, Yang KC, Mehta MP. Angiogenic blockade and radiotherapy in hepatocellular carcinoma. Int J Radiat Oncol Biol Phys 2010 Feb 2. [PMID 20133077]
- National Cancer Institute. Common Terminology Criteria for Adverse Events v3.0 (CTCAE). Cancer Therapy Evaluation Program (CTEP), 2006.
- Bayer AG. Leverkusen, Germany. Nevaxar (sorafenib). Highlights of prescribing information.
- Li M, Srinivas S. Acute pancreatitis associated with sorafenib. South Med J 2007; 100:909-11. [PMID 17902294]
- Amar S, Wu KJ, Tan WW. Sorafenib-induced pancreatitis. Mayo Clin Proc 2007; 82:521. [PMID 17418082]
- Saadati H, Saif MW. Sorafenib-induced acute pancreatitis. JOP. J Pancreas (Online) 2010; 11:283-4.
- Ueda T, Takeyama Y, Yasuda T, Matsumura N, Sawa H, Nakajima T, Kuroda Y. Vascular endothelial growth factor increases in serum and protects against the organ injuries in severe acute pancreatitis. J Surg Res 2006; 134:223-30. [PMID 16488441]
- Pierce GF, Mustoe TA, Lingelbach J, Masakowski VR, Griffin GL, Senior RM, Deuel TF. Platelet-derived growth factor and transforming growth factor-beta enhance tissue repair activities by unique mechanisms. J Cell Biol 1989; 109:429-40. [PMID 2745556]

