Keywords
Bariatric surgery; Laparoscopic adjusted gastric banding; High risk pregnancy; Pregnancy complication
Introduction
Worldwide obesity has doubled since 1990 [1]. Overall, pregnant obese women are at higher risk of obstetrical complications [2-5]. In order to reduce these complications, it is recommended to lose weight prior to conception. Bariatric surgery is an option for women with a BMI of 40 or more, or a BMI of 35 or more in combination with specific comorbidities. The impact of bariatric surgery on the pregnancy outcome compared to the general population is less well studied. Besides the maternal and neonatal advantages and/or complications, bariatric surgery implies some procedure specific complications. We will focus on Laparoscopic Adjusted Gastric Banding (LAGB) specific complications.
Case Report
A 21-year old woman, G1P0, was admitted to our University Hospital at 33 weeks and 2 days of gestational age with a 1 week history of nausea and vomiting. Two years before, in 2013, the patient underwent laparoscopic adjusted gastric banding (LAGB) elsewhere for morbid obesity with a BMI of 39.3. Postoperatively her BMI dropped to 23.5. The medical history was limited to the LAGB.
Before transfer to our hospital, the patient had already been admitted for 1 week in a general hospital. Because of intractable vomiting, the band was loosened, without improvement of her symptoms. Blood sample showed doubled transaminases. Serology was negative for hepatitis A, B and C virus, Epstein Barr virus and cytomegalovirus. Abdominal ultrasound revealed distention of the stomach; the liver and biliary ducts were normal. The abdominal ultrasound was repeated after 3 days and revealed no new findings. Obstetric ultrasound there was suspicion of intra-uterine growth restriction (IUGR) and anhydramnion. Finally she was transferred to our hospital because of persistent vomiting, the increased transaminases of unknown origin, and the suspected IUGR with anhydramnion.
At the time of transfer, there was no vaginal blood or fluid loss, fetal movements were normal and there were no complaints of itching. The vital parameters were normal (blood pressure 117/69 mmHg, heart rate 58 beats per minute, temperature 36.5°C). She looked pale. She had a BMI of 28,7. Clinical examination of the abdomen revealed epigastric tenderness and a mass in the left hypochondrium. Knee reflexes were normal and there was no edema. The test for premature rupture of the membranes was negative. Cervical length was 22 mm. Laboratory examination revealed increased transaminases (AST 106 U/L (0-31), ALT 140 U/L (7-31)), bilirubine (4.3 mg/dl (0.2-1.3)), uric acid (10.6 mg/dl (2.4-5.7)) LDH (273 U/L (105-233)), CRP (24.4 mg/dl (<5.0)) and thrombocytopenia (128 x 103/μL (171-374)). Cardiotocography (CTG) was normal (baseline 140 beats per minute, variable, accelerative, no decelerations, 2 irregular contractions per 10 minutes). The estimated fetal weight was 1960 grams (corresponding with P25). Doppler examination of the umbilical artery, medial cerebral artery and venous duct were all normal. The anhydramnion was confirmed.
The differential diagnosis consisted of HELLP, acute fatty liver (AFL) or a complication of the gastric band. The woman was admitted for observation. Intravenous fluid therapy was started (3 L/24 h). Metoclopramide was administered intravenously. The urine was collected for 24 h. Because of gestational age, betamethasone 12 mg was administered twice intramuscularly, with an interval of 24 hours.
The patient was approached multidisciplinary. We consulted our colleagues gastroenterologists, surgeons, and the obstetric anaesthesiologist. The differential diagnosis of the gastroenterologists consisted of HELLP syndrome and pathology of the biliary tract, despite normal ultrasound examination in the referral hospital. For this reason the abdominal ultrasound was repeated. Besides the distention of the stomach and physiologic hydronephrosis, no new abnormalities were revealed.
Because of clinical deterioration (increased nausea, vomiting and epigastric pain) and biochemical deterioration (AST 138 U/L, ALT 198 U/L, platelets 93 x 103/μL) a primary cesarean section was performed based on the suspicion of HELLP syndrome. The obstetric anesthesiologist administered ranitidine, sodium and sodium citrate as premedication, then a combined spinal-epidural technique (CSE) was performed. A daughter was born, Apgar score 9 after 1 minute and 10 after 10 minutes, birth weight 2155 grams (corresponding with P25). She was admitted to the neonatal intensive care unit (NICU) (Figure 1).
The epigastric pain, nausea and vomiting persisted after the Cesarean section. In consultation with the surgical department, a nasogastric tube was placed. More than one liter of fluid, looking like coffee ground, was removed and the patient improved slightly. Vomiting reoccurred subsequent to the (patient guided) removal of the nasogastric tube. An esophagogastroduodenoscopy (EGD) was performed and showed serious band slipping (picture 1). The patient was planned for urgent laparoscopy (Figure 1).
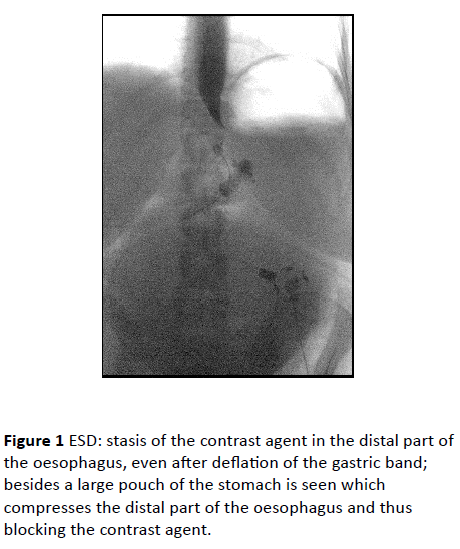
Table 1 Overview case reports
At laparoscopy, a gigantic edematous stomach was seen (size comparable to a 40 weeks gravid uterus), as well as ascites. At exploration, not only a slipping of the gastric band was seen, there was also a torsion of the stomach. After detorsion and removal of the gastric band, more than 3 liter of fluid was removed through the nasogastric tube. After a short stay in the intensive care unit, the patient was transferred to the maternity. The postoperative phase was uneventful. The nasogastric tube could be removed 2 days after the surgery. The oral intake could be gradually expanded without problems. One month later, the patient was seen in the outpatient clinic without digestive symptoms.
Literature
Worldwide obesity has doubled since 1990 [1]. In 2014, 39% of adults aged 18 years and older were overweight, and 13% were obese. Overall, pregnant obese women are at higher risk of obstetrical complications [2-5]. There is a significant increased risk of namely fertility problems, miscarriage, gestational diabetes, gestational hypertension, preeclampsia, macrosomia, caesarean section and its related complications such as haemorrhage, wound infection and anaesthetic complications.
In order to reduce these complications, it is recommended to lose weight prior to conception. First of all, physical activity is encouraged and diet recommendations are provided [5]. Bariatric surgery is an option for women with a BMI of 40 or more, or a BMI of 35 or more in combination with specific comorbidities. There are three types of bariatric procedures: the restrictive procedure (vertical banded gastroplasty, laparoscopic adjusted gastric banding (LAGB), sleeve gastrectomy), the malabsorptive procedure (jejunoileal bypass, biliopancreatic diversion, biliopancreatic diversion with duodenal switch) and the combination of both procedures (gastric bypass) [6]. Buchwald et al. did a survey in 50 nations in order to provide global bariatric surgery data [7]. Trends in procedures in Europe from 2003 to 2011 showed a decrease in LAGB and an increase in gastric bypass and sleeve gastrectomy. Some hypotheses can be provided for this shift in procedures: it has become clear that LABG on the long term leads to less weight loss and more complications in comparison with a gastric bypass or sleeve gastrectomy; also surgeons like to try out innovative procedures. A Cochrane review assessed the effect of the bariatric procedure and the control of comorbidities [8]. The weight loss is similar for gastric bypass and sleeve gastrectomy, and both of these procedures had better outcomes than LAGB. Adverse event rates and reoperation rates were generally poorly reported. One study on more than 700 patients reports a reoperation rate of 23% after LAGB at 7 years of follow up [9]. Overall, the long term weight loss after bariatric surgery is greater than 60% and stabilization is seen 2 years after surgery [10]. For this reason it’s recommended to postpone a pregnancy for at least 12-18 months after surgery.
Despite the assumed reduction in the aforementioned obstetrical risks, there is an augmented risk of intra-uterine growth retardation. Several case reports and small studies have identified late complications of previous surgery, including intestinal obstruction and gastro-intestinal haemorrhage [11]. There should be a high index of suspicion for those complications if pregnant women who have had bariatric surgery present with abdominal symptoms. A trend towards lower mean birth weight is seen in pregnancies subsequent to bariatric surgery. Moreover there are fewer large for gestational age.
The impact of bariatric surgery on the pregnancy outcome compared to the general population is less well studied. The best known complication is nutritional deficiency after gastric bypass, but there is a gap in the knowledge concerning pregnancy outcomes [12]. Belogolovkin et al conducted a population-based retrospective cohort study to investigate the association between bariatric surgery and pregnancy-related outcomes among mothers and neonates [13]. Their study showed that non-obese mothers with prior bariatric surgery were more likely to have anemia, chronic hypertension, endocrine disorders, and IUGR; whereas obese mothers without prior bariatric surgery were at greater risk of having gestational diabetes, chronic hypertension, macrosomic infants, and prolonged hospital stay as compared to non-obese mother without prior bariatric surgery. Unfortunately, the type of bariatric surgery was not specified.
In particular for LAGB, data on pregnancy outcomes are limited [3]. In a subanalysis of a systematic review by Galazis et al, LAGB did not appear to increase the risk of IUGR as was seen in other bariatric surgery procedures [14]. Moreover, Dixon et al provided a prospective study of 79 women who became pregnant after LAGB. The pregnancy outcomes (pregnancy induced hypertension (PIH), gestational diabetes, stillbirths, preterm deliveries, IUGR, and high birth weight) were consistent with general community outcomes [15].
These results were confirmed in 22 pregnancies after LAGB by the same studygroup [16]. In 15 of the 22 pregnancies, band adjustments were made. Lapola and colleagues however revealed that the incidence of PIH, pre-eclampsia, caesarean section, preterm birth, large for gestational age, spontaneous abortion, and NICU admission was higher in post-LAGB pregnancies than in normal weight pregnancies [17]. In conclusion, knowledge on the pregnancy outcomes of women who underwent LAGB is limited, but it seems that LABG is the preferred type of bariatric surgery for women with pregnancy desire. A multidisciplinary approach is recommended for pregnant women who have undergone LAGB. In order to avoid nutritional deficiencies, it is recommended to assess the need to adjust the gastric band during pregnancy so the woman can eat enough to support normal fetal growth [12,15].
Besides the maternal and neonatal advantages and/or complications, bariatric surgery implies some procedure specific complications. We will focus on LAGB specific complications.
The reported incidence of band slippage varies between 1 and 22% [18]. There are two subtypes of band slippage: anterior or posterior gastric prolapse. In anterior gastric prolapse, the band is moving cranially and it creates a critical angle between the stomach pouch and esophagus, causing obstruction. In posterior gastric prolapse, the stomach body is moving cranially, creating a new large stomach pouch. The posterior form is more common than the anterior form. Both types of slippage cause obstruction and are characterized by food intolerance, epigastric pain, nausea and vomiting. Removal of the band is necessary in order to avoid strangulation of the stomach.
Acute stomach obstruction can occur immediately after the LABG procedure or after band adjustment. The incidence is 14% and the treatment consists of removing fluid from the port. Band erosion occurs in 1% of the cases and is caused by wall ischemia, pressure necrosis or infection. The treatment is removal of the band and closure of a possible stomach ulcer. In case of band or balloon leakage, the goal of food restriction is not attained and the band has no use. Pouch or esophagal dilatation arise when food is consumed faster than it can empty from the pouch.
Haward and colleagues compared the incidence of revisional procedures in pregnant and non-pregnant women with LAGB [19]. The type of complication was not statistically different between the groups. It seems unlikely that pregnancy influences the need for LAGB revision. However, a shorter period between the LAGB procedure and the pregnancy may put the patient at a greater risk of complications. To date, only 5 cases on band slippage during pregnancy have been published and only one case reports on gastric torsion [20-25]. The 6 cases are summarized in Table 1. In the case report of Policiano et al, the low Apgar score could be explained by the use of pethidine prior to the caesarean section [24].
| Author |
Year |
Patient |
BMI |
Symptoms |
Lab |
Pelvic examination |
Fetal |
Mode of
delivery |
Neonate |
LAGB |
Time since LAGB |
Postpartum |
| Policiano et al. |
2013 |
37y, G1P0, 30w
no comorbidities |
19 |
nausea reflux vomiting
abdominal pain |
hyperglycaemia
metabolic acidosis
ketonurie
WBC normal
liver normal
pancreas normal |
50% effaced
1cm dilated |
abnormal CTG |
urgent
C-section |
Boy
AS 4/8
1870gr |
hemoperitoneum during C-section,
gastric rupture,
gastric band dislodged down
removal band,
partial gastrectomy |
/ |
Uneventful
Discharged day 8 |
| Kirshtein et al. |
2010 |
34y, G?
36w
no comorbidities |
26,6 |
nausea, reflux, vomiting, abdominal pain |
n.a. |
n.a. |
IUGR |
vaginal 4w after revision LAGB |
Boy
3442gr |
removal laparoscopically |
9 m |
n.a. |
| Suffee et al. |
2012 |
29y, G2P1,
30w
comorbidities unknown |
n.a. |
dysphagia |
hypokalaemia |
closed |
Normal CTG
EFW >P10 |
n.a. |
n.a. |
removal laparoscopically |
5y |
n.a. |
| Denino et al. |
2011 |
29y, G1P0,
12w
comorbidities unknown |
n.a. |
poor oral intake
nausea
vomiting |
Potassium 2,9 meq/L |
n.a. |
n.a. |
n.a. |
n.a. |
removal laparoscopically |
8 m |
n.a. |
| Pilone et al. |
2010 |
25y,
no comorbidities |
22,2 |
Hyperemesis gravidarum
Sings of malnutrition |
n.a. |
n.a. |
Normal condition |
n.a. |
n.a. |
removal laparoscopically |
3 y |
n.a. |
| Mohamed et al. |
2012 |
25y, G1P0,
29w,
comorbidities unknown |
n.a. |
vomiting
abdominal pain |
reduced albumin
WBC normal
ALT, AST raised |
n.a. |
IUGR |
Elective C-section 32w |
Boy
1875gr |
removal by laparotomy
180° gastric torsion , viable after detorsion |
n.a. |
n.a. |
van Wessel
et al. |
2015 |
21y, G1P0, 33w
no comorbidities |
/ |
nausea
vomiting
epigastric pain |
platelets low
ALT, AST raised
CRP slightly raised |
Cervix length 22mm |
EFW P25 |
Urgent C-section |
Girl
2155gr
AS 9/10 |
slipping and gastric torsion removal laparoscopically 3 days after C-section |
8y |
Discharged 6days postpartum |
Table 1: Overview case reports
In the case report of Suffee et al, the band slippage occurred 5 years after the surgical procedure [25]. In that interval, there was an uncomplicated pregnancy and delivery. The gastric band was deflated at 18 weeks of gestation because of vomiting. Nevertheless, slippage occurred at 30 weeks of gestational age. In the case report of Denino and colleagues, the band slippage occurred at 12 weeks of gestational age [20]. Initially, the symptoms were assigned to hyperemesis gravidarum. The fluid in the band was removed without improvement. An EGD demonstrated an altered gastric anatomy with tight folding in the mid-portion of the body, the antrum was difficult to visualise. The decision was made to perform a diagnostic laparoscopy. Eventually the band was removed.
the case report of Pilone and colleagues, the band slippage occurred at 13 weeks of gestational age because of hyperemesis gravidarum [23]. The band was already deflated and the hyperemesis gravidarum was managed conservatively until 13 weeks of gestation. She was admitted to the hospital because of a weight loss of 12 kg from the beginning of the pregnancy. The patient refused a gastroscopy. Abdominal ultrasound revealed dilatation of the pouch, proximal to the band. Laparoscopic evaluation showed a large pouch proximal to the band, slipped until the antrum, where an area of fibrosis seemed to cause stenosis. The band was removed.
Mohamed and colleagues are the only authors reporting on gastric torsion [22]. In this case the gastric band was already deflated once the pregnancy was discovered. Because of persistent vomiting, an abdominal ultrasound and an EGD were performed. These examinations did not reveal any abnormalities. Because of the complaints and the IUGR, it was decided multidisciplinary to perform an elective caesarean section. Post-caesarean, the patient deteriorated. A mechanical obstruction was suspected. An urgent laparotomy was performed and revealed a dislodged gastric band as well as a gastric torsion. The gastric band was removed and the stomach was viable after the detorsion.
In conclusion, our case report is relatively unique because of the combination of band slippage and gastric torsion in pregnancy after LAGB. We found only one case report on the same topic. Five other case reports published on band slippage during pregnancy. The data to date indicate that pregnancy after bariatric surgery appears to reduce the risk of several complications related to obesity. However, women who become pregnant after bariatric surgery may constitute a unique obstetrical population with an increased risk for IUGR. The risk for IUGR is less in case of LAGB compared to other bariatric procedures. LAGB seems the method of choice in obese women planning to become pregnant. The LAGB procedure related complications are rare. Although pregnancy is not a predisposing factor for these complications, special care should be provided to women pregnant after LAGB. In case of nausea and vomiting after LAGB, the LAGB procedure related complications should be included in the differential diagnosis [26].
References
- Obesity and overweight, fact sheet 311(2015) WHO, USA
- American College of Obstetricians and Gynecologists (2005) ACOG Committee Opinion number 315, September 2005. Obesity in pregnancy. ObstetGynecol 106: 671-675.
- Carelli AM, Ren CJ, Youn HA, Friedman EB, Finger AE, et al. (2011) Impact of laparoscopic adjustable gastric banding on pregnancy, maternal weight, and neonatal health. ObesSurg 21:1552-1558.
- Dao T, Kuhn J, Ehmer D, Fisher T, McCarty T (2006) Pregnancy outcomes after gastric-bypass surgery. Am J Surg 192: 762-766.
- Mission JF, Marshall NE, Caughey AB (2013) Obesity in pregnancy: a big problem and getting bigger. ObstetGynecolSurv 68: 389-399.
- Beard JH, Bell RL, Duffy AJ (2008) Reproductive considerations and pregnancy after bariatric surgery: current evidence and recommendations. ObesSurg 18: 1023-1027.
- Buchwald H, Oien DM (2013) Metabolic/bariatric surgery worldwide 2011. ObesSurg 23: 427-436.
- Colquitt JL, Pickett K, Loveman E, Frampton GK (2014) Surgery for weight loss in adults. Cochrane Database Syst Rev 8: CD003641.
- Van Nieuwenhove Y, Ceelen W, Stockman A, Vanommeslaeghe H, Snoeck E, et al. (2011) Long-term results of a prospective study on laparoscopic adjustable gastric banding for morbid obesity. ObesSurg 21: 582-587.
- Bebber FE, Rizzolli J, Casagrande DS, Rodrigues MT, Padoin AV, et al. (2011) Pregnancy after bariatric surgery: 39 pregnancies follow-up in a multidisciplinary team. ObesSurg 21: 1546-1551.
- American College of Obstetricians and Gynecologists1 (2009) ACOG practice bulletin no. 105: bariatric surgery and pregnancy. ObstetGynecol 113: 1405-1413.
- Conrad K, Russell AC, Keister KJ (2011) Bariatric surgery and its impact on childbearing. NursWomens Health 15: 226-233, quiz 234.
- Belogolovkin V, Salihu HM, Weldeselasse H, Biroscak BJ, August EM et al. (2012) Impact of prior bariatric surgery on maternal and fetal outcomes among obese and non-obese mothers. Arch GynecolObstet 285: 1211-1218.
- Galazis N, Docheva N, Simillis C, Nicolaides KH (2014) Maternal and neonatal outcomes in women undergoing bariatric surgery: a systematic review and meta-analysis. Eur J ObstetGynecolReprodBiol 181: 45-53.
- Dixon JB, Dixon ME, O'Brien PE (2005) Birth outcomes in obese women after laparoscopic adjustable gastric banding. ObstetGynecol 106: 965-972.
- Dixon JB, Dixon ME, O'Brien PE (2001) Pregnancy after Lap-Band surgery: management of the band to achieve healthy weight outcomes. ObesSurg 11: 59-65.
- Lapolla A, Marangon M, Dalfrà MG, Segato G, De Luca M, et al. (2010) Pregnancy outcome in morbidly obese women before and after laparoscopic gastric banding. ObesSurg 20: 1251-1257.
- Lim RB, Blackburn GL, Jones DB (2010) Benchmarking best practices in weight loss surgery. CurrProblSurg 47: 79-174.
- Haward RN, Brown WA, O'Brien PE (2011) Does pregnancy increase the need for revisional surgery after laparoscopic adjustable gastric banding? ObesSurg 21: 1362-1369.
- DeNino WF, Zubarik RS, Forgione PM (2011) Laparoscopic gastric band slippage diagnosed with esophagogastroduodenoscopy in a 12-week gestation nulliparous patient. SurgObesRelat Dis 7: 225-226.
- Kirshtein B, Lantsberg L, Mizrahi S, Avinoach E (2010) Bariatric emergencies for non-bariatric surgeons: complications of laparoscopic gastric banding. ObesSurg 20: 1468-1478.
- Mohamed D, El Hadi A, Smajer B (2012) Stomach torsion in pregnancy as a complication of laparoscopic adjustable gastric banding. J Surg Case Rep 2012: 1.
- Pilone V, Di Micco R, Monda A, Villamaina E, Gentile M, et al. (2012) P. LAGB in pregnancy: slippage after hyperemesis gravidarum. Report of a case. Ann ItalChir 83: 429-432.
- Policiano C, Rocha P, Catanho MC, Pinto L, Valentim-Lourenco, et al. (2013) Acute fetal asphyxia after gastric rupture in a pregnant patient with a gastric band. ActaObstetGynecolScand 92: 1419-1421.
- Suffee MT, Poncelet C, Barrat C (2012) Gastric band slippage at 30 weeks' gestation: diagnosis and laparoscopic management. SurgObesRelat Dis 8: 366-368.
- Kominiarek MA (2011) Preparing for and managing a pregnancy after bariatric surgery. SeminPerinatol 35: 356-361.

