Keywords
Antineoplastic Agents; Biological Therapy; gemcitabine; Pancreatic Neoplasms
What Did We Know Before the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting?
Pancreatic cancer is a lethal malignancy which is affecting many patients in the Western mostly countries. Unfortunately, there is often lack of warning signs or early symptoms; therefore, more than 2/3 of patients present at a late stage at the time of diagnosis [1]. Advanced disease precludes cure, so symptoms palliation, quality of life and prolongation of life by a few months are the aims of treatment. So far, gemcitabine monotherapy, and less so its combination with other drugs, was the only accepted treatment worldwide. The limited options were recently enriched, after the results of a large study that demonstrated survival benefit of patients with advanced pancreatic cancer treated with combination of oxaliplatin, irinotecan and 5-fluorouracil, though this regimen was well tolerated only by very fit patients, which is not often the case in this disease [2].
Since the efficacy of most cytotoxis is at least very modest, if not disappointing, the efforts lie on the addition of biological or novel agents to gemcitabine, hoping to find a pivotal pathway which may play role in this disease [3]. In the following paragraphs we will discuss the main results and findings of research on the management of advanced pancreatic cancer.
What Did We Learn at the 2011 ASCO Annual Meeting?
Combining Cytotoxics
Firstly, as far as the combination of gemcitabine with other conventional cytotoxics is concerned, Abstracts #4029, #4040 and #4007 address the role of the antimetabolite S-1 in pancreatic cancer. The design of these studies and their results are demonstrated in Table 1 [4, 5, 6].
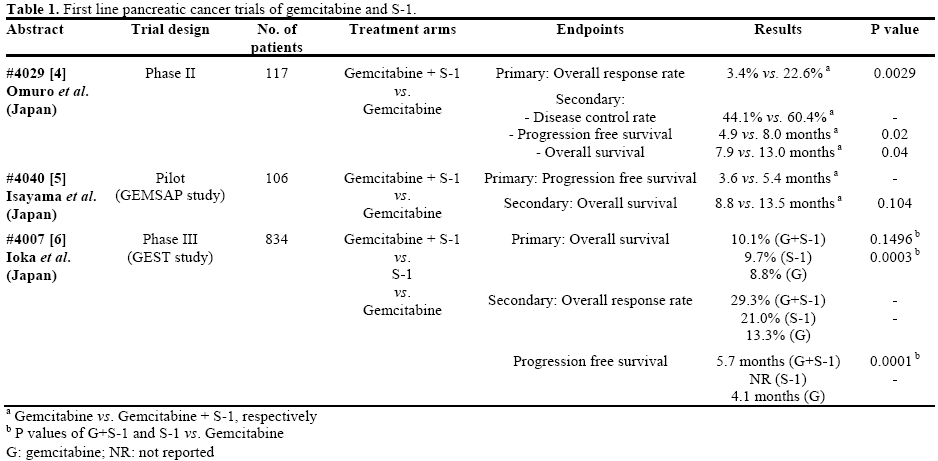
Commenting on the role of S-1 on the whole after the above results, we could first accept that S-1 is an active fluoropyrimidine in pancreatic cancer which is not inferior to gemcitabine; so, S-1 could be another option. Furthermore, the combination of gemcitabine with S-1 offered a better quality of life than single agent gemcitabine or S-1. Nevertheless, the design of these studies does not answer definitely whether the combination is indeed better than monotherapies, thus more research is needed. We would suggest that since S-1 is only available in Japanese patients, and we often see racial and interethnic genomic differences, the results should be reproduced to other continents as well.
Targeting the Epidermal Growth Factor and Insulin Growth Factor-1 Pathways
Based on the modest clinical benefit, but statistically significant, by adding erlotinib to gemcitabine, a new phase II study was presented at the ASCO 2011 Annual Meeting exploring the benefit of dual epidermal growth factor receptor (EGFR) inhibition by combining erlotinib, panitumumab and gemcitabine (Abstract #4030) [7]. There was a significant improvement in overall survival by 4.4 months (8.4 vs. 4.0; P=0.077) though there was also a very high increase in nonhematological toxicity (61% vs. 30%). The study met its primary endpoint, thus combining panitumumab, gemcitabine, and erlotinib may be a useful option in pancreatic cancer providing the result will be confirmed in a large randomized phase III study and some kind of biomarker will select patients most likely to respond and tolerate this regimen (K-ras studies are ongoing).
Other biological tested in this setting, are agents targeting the insulin growth factor-1 (IGF-1) pathway which is often upregulated in pancreatic cancer. IGF receptor-1 (IGFR-1) antibodies such as the MK0646 and ganitumab were tested. With regards to MK0646, it was shown in a phase II, three-arm study that combination of MK0646 with gemcitabine produced a higher progression free survival rate as compared to MK0646-gemcitabine-erlotinib or gemcitabine-erlotinib, and a satisfactory partial response rate 20% (vs. 25% and 10%, respectively) though there were no differences in overall survival between arms (Abstract #4026) [8].
Ganitumab, a fully human IGFR-1 antibody, showed in a phase II study (Abstracts #4049 and #4041) that can increase the efficacy and survival of patients with advanced pancreatic cancer when combined to gemcitabine, therefore the ongoing phase III GAN P3 study will define its exact benefit in this disease[9, 10].
Gemcitabine with Other Novel Molecular Agents in Phase I/II Level
More research on biological agents is ongoing. There were quite a few phase I studies that tested the safety and tolerability of various agents targeting molecules overexpressed in pancreatic cancer in combination with gemcitabine, listed in Table 2 [11, 12, 13].

Apart from the phase I/II studies listed in Table 2, it would be worth mentioning the phase Ib study that evaluated the hedgehog pathway inhibitor IPI-926 in combination with gemcitabine (Abstract #4114) [14]. The hedgehog ligand is produced by cancer stromal cells and contributes to the hedgehog signaling (by interacting with patched and smoothened molecules) which regulated stroma and tumor microenvironment and plays role in tumor growth and survival (Figure 1). IPI-926 is an oral small molecule antagonist of smoothened protein. This study demonstrated the combination of IPI-926 with gemcitabine was safe and well-tolerated. Dosing of IPI-926 ranged from 110 mg to 160 mg, with partial responses observed at each of them (a total of 31% of patients demonstrated radiological partial response and 50% of patients a decrease of CA 19-9 by more than 50%). Based on these finding a phase II study testing IPI-926 160 mg with gemcitabine is now actively recruiting patients and the results will be much anticipated.
Figure 1. The hedgehog pathway and the interaction of tumor cells with stromal cell (left); the inhibitor of the smoothened (Smo) molecule, IPI-926
(chemical form on the right) (Adapted from the original abstract poster presented at the 2011 ASCO Annual Meeting [14]).
Unfortunately, but not unexpectedly, the combination of sorafenib with gemcitabine, showed no survival benefit in a phase III study (Abstract #4028) [15].
Discussion
The progress in the treatment of pancreatic cancer has been disappointing for many decades. We still observe our patients passing away quite early after the diagnosis, without having improved much of their suffer. Despite this groom reality, there is a sense of change in the air. First, with the fact that drugs other than gemcitabine, such as the combination of 5- fluorouracil, irinotecan and oxaliplatin (FOLFIRINOX), can significantly improve survival, especially in a subgroup of very fit patients. Second, with the evidence presented above that S-1, is equal to gemcitabine, at least at the Japanese population that it was tested, and the two drugs may well combine together with some improvement of results. We may acknowledge that while most of the novel agents that initially excite us, they prove at the end less effective in the clinical setting, it is important to explore the molecular basis of the disease and the reasons which lie behind progression and drug resistance. Therefore, from the many targeted agents that are presented here, it seems that the most promising might be the hedgehog inhibitor IPI-926 which aims to block processes at the stroma microenvironment related to angiogenesis, disease progression and refractoriness to treatment. Hopefully, we may find at the near future the effective treatment which has also to be costeffective in order to allow use it broadly.
Conflict of interest
The authors declare no conflicts of interest
References
- Strimpakos A, Saif MW, Syrigos KN. Pancreatic cancer: from molecular pathogenesis to targeted therapy. Cancer Metastasis Rev 2008; 27(3):495-522.
- Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364(19):1817-1825.
- Strimpakos AS, Syrigos KN, Saif MW. The molecular targetsfor the diagnosis and treatment of pancreatic cancer. Gut Liver 2010;4(4):433-449.
- Omuro Y, Ikari T, Ishii H, Ozaka M, Suyama M, Matsumura Y,et al. A randomized phase II study of gemcitabine plus S-1 versus gemcitabine alone in patients with unresectable pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):4029.
- Isayama H, Nakai Y, Sasaki T, Sasahira N, Hirano K, Tsujino T,et al. The final analysis of a multicenter randomized controlled trialof gemcitabine (G) alone versus gemcitabine and S-1 combination therapy (GS) in patients with unresectable advanced pancreatic cancer (PC): GEMSAP study. J Clin Oncol 2011; 29(Suppl.):4040.
- Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Fukutomi A, Sugimori K, et al. Randomized phase III study of gemcitabine plusS-1 (GS) versus S-1 versus gemcitabine (GEM) in unresectable advanced pancreatic cancer (PC) in Japan and Taiwan: GEST study. J Clin Oncol 2011; 29(Suppl.):4007.
- Kim GP, Foster NR, Salim M, Flynn PJ, Moore DF, Zon R, etal. Randomized phase II trial of panitumumab, erlotinib, andgemcitabine (PGE) versus erlotinib-gemcitabine (GE) in patients with untreated, metastatic pancreatic adenocarcinoma. J Clin Oncol 2011; 29(Suppl.):4030.
- Javle MM, Varadhachary GR, Fogelman DR, Shroff RT,Overman MJ, Ukegbu L, et al. Randomized phase II study of gemcitabine (G) plus anti-IGF-1R antibody MK-0646, G pluserlotinib (E) plus MK-0646 and G plus E for advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):4026.
- Lu J, Deng H, Tang R, Hsu C, Kindler HL, Fuchs CS, et al. Exposure-response (E-R) analysis to facilitate phase III (P3) doseselection for ganitumab (GAN, AMG 479) in combination with gemcitabine (G) to treat metastatic pancreatic cancer (mPC). J Clin Oncol 2011; 29(Suppl.):4049.
- McCaffery I, Tudor Y, Deng H, Tang R, Badola S, Kindler HL,et al. Effect of baseline (BL) biomarkers on overall survival (OS) inmetastatic pancreatic cancer (mPC) patients (pts) treated with ganitumab (GAN; AMG 479) or placebo (P) in combination with gemcitabine (G). J Clin Oncol 2011; 29(Suppl.):4041.
- Aglietta M, Barone C, Sawyer MB, Moore MJ, Miller WH, Bagal C, et al. Final toxicity results of a phase I dose-escalation trial of tremelimumab (CP-675206) in combination with gemcitabine in chemotherapy-naive patients (pts) with metastatic pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):4081.
- Wolpin BM, O'Reilly EM, Ko Y, Blaszkowsky LS, Rarick MU,Rocha Lima C. MS, et al. Global, multicenter, open-label, randomized phase II trial comparing gemcitabine (G) with. G plusAGS-1C4D4 (A) in patients (pts) with metastatic pancreatic cancer(mPC). J Clin Oncol 2011; 29(Suppl.):4031.
- Ramanathan RK, Chadha M, Gressler V, Shah S, Loury D, Hamdy A, et al. Phase I/II pharmacokinetic and pharmacodynamic study of PCI-27483, a coagulation factor VIIa (FVIIa) inhibitor, inpatients with advanced pancreatic cancer receiving treatment with gemcitabine. J Clin Oncol 2011; 29(Suppl.):e14610.
- Stephenson J, Richards DA, Wolpin BM, Becerra C, Hamm JT, Messersmith WA, et al. The safety of IPI-926, a novel hedgehog pathway inhibitor, in combination with gemcitabine in patients (pts) with metastatic pancreatic cancer. J Clin Oncol 2011;29(Suppl.):4114.
- Goncalves A, Viret F, Frannois E, Dahan L, Perrier H, Lamy R,et al. BAYPAN study: A double-blind, phase III randomized trial of gemcitabine plus sorafenib versus gemcitabine plus placebo inpatients with advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):4028.


