Keywords
capecitabine; lapatinib; Pancreatic Neoplasms; S-1; Treatment Failure
Abbreviations
ASCO: American Society of Clinical Oncology; FOLFIRI: irinotecan with 5-FU and folinic acid; FOLFOX: 5-FU plus folinic acid plus oxaliplatin; HER2: human epidermal growth factor receptor 2; TKI: tyrosine kinase inhibitor
INTRODUCTION
Pancreatic cancer remains a malignancy of poor prognosis as overall survival has shown little improvement despite recent advances in therapeutics. With an estimated total of approximately 276,000 deaths in 2011 on a worldwide basis [1], pancreatic cancer constitutes a therapeutic challenge in current oncology practice. Gemcitabine monotherapy and its combination with erlotinib represent the current goldstandard treatment in advanced pancreatic adenocarcinoma with only modest benefit [2]. After failure of gemcitabine-based regimens, there are limited options available for second-line treatment, mainly because few large clinical trails have been conducted in this field [3]. Therefore, any new developments in this setting are of particular clinical interest.
What Did We Know Before the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting?
Second-line chemotherapy offers better survival rates as compared to best supportive care, since Oettle et al. [4] showed benefit with the use of 5-FU/folinic acid/oxaliplatin (FOLFOX) as compared to offering best supportive care alone (median survival of secondline therapy: 21 vs. 10 weeks). In the landmark Charité Onkologie Clinical (CONKO)-003 trial, Pelzer et al. [5] demonstrated that the addition of oxaliplatin to 5- FU and leucovorin significantly improves overall survival and progression-free survival. Therefore, it is suggested that FOLFOX become the standard secondline treatment.
According to recent retrospective studies on taxanes, paclitaxel monotherapy shows mild efficacy with manageable toxicity in the second-line setting [6], as do docetaxel-based regimens [7]. Another agent also targeting microtubule dynamics, the halichondrin B analog eribulin mesylate, seems able to prolong stable disease with good tolerability [8]. Regarding irinotecan, Oh et al. [9] demonstrated that the combination of this agent with oxaliplatin offers a 50% disease control rate with a good toxicity profile. The combination of irinotecan with 5-FU and folinic acid (FOLFIRI) showed modest activity [10] in a randomized phase II study by Yoo et al. and these results were verified by a most recent retrospective study by Neuzillet et al. [11], with a 44.3% response rate. Ko et al. [12] showed that liposome irinotecan (PEP02), a nanoparticle formulation of irinotecan with better pharmacokinetics and tumor distribution, may also be a promising option for gemcitabine-refractory patients, offering a median progression-free survival of 9 weeks.
The efficacy of capecitabine in the second-line treatment of pancreatic adenocarcinoma has been explored in various combinations. Capecitabine monotherapy has been described as a safe option in an effort to prolong survival [13]. Its efficacy has been suggested to be correlated with thymidine phosphorylase and dihydropyrimidine dehydrogenase levels [14]. A 2008 phase II study showed that the combination of capecitabine plus oxaliplatin is active in patients with good performance status that have shown some response to first-line gemcitabine in the past (progression-free survival: 9.9 weeks) [15]. The clinical efficacy of this regimen was similar to that of the capecitabine-gemcitabine doublet in the Boeck et al. trial [16]. Combinations of capecitabine with celecoxib [17] or docetaxel [18] have also exhibited modest activity and tolerable toxicity after gemcitabine failure.
S-1 is an oral fluoropyrimidine that has been mostly investigated in Japanese populations (Figure 1). S-1 monotherapy has been mostly reported as well tolerated but only marginally effective in the secondline setting with moderate disease control rates [19, 20]. However, a most recent phase II study showed a relatively high disease control rate and marked decrease in tumor markers [21]. Combinations of S-1 plus irinotecan [22] or cisplatin [23] seem feasible with manageable toxicity warranting further investigation. Targeted therapies have also been evaluated in the second-line treatment, mostly with poor results. Monotherapy with sunitinib [24], everolimus [25], and bevacizumab [26] have shown inadequate antitumor activity, as have the combinations of bevacizumab with erlotinib [27] or docetaxel [26]. The combination of S- 1 with lapatinib has shown some promising activity in in vitro and in vivo studies [28]. Finally, erlotinib plus capecitabine seems to be a safe and active treatment option according to a phase II trial [29].
Figure 1. S-1: an oral fluoropyrimidine (adapted from Saif [35]).
What Did We Learn at the 2011 ASCO Annual Meeting?
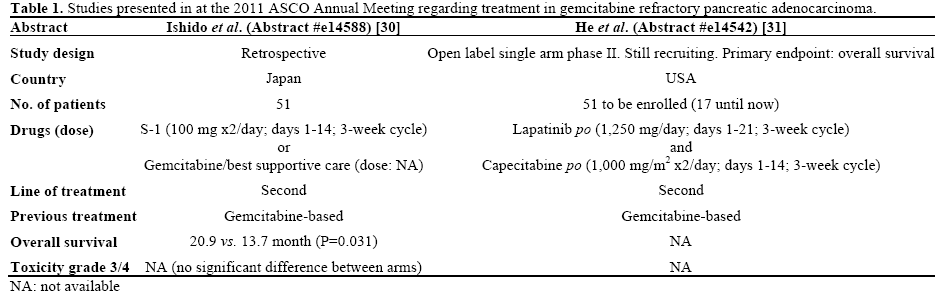
With regard to the treatment of gemcitabine-refractory pancreatic adenocarcinoma, two important abstracts were presented at the 2011 ASCO Annual Meeting (Table 1).
S-1 in Second-Line Therapy
Ishido et al. (Abstract #e14588) [30] conducted a retrospective study to evaluate the efficacy and safety of S-1 as second-line chemotherapy after failure of gemcitabine. The 51 enrolled patients were divided in two groups: those receiving S-1 monotherapy (26 patients) and those continuing to receive gemcitabine plus best supportive care (25 patients). There was a statistically significant difference between the two groups in overall survival (20.9 vs. 13.7 months; P=0.031) and in survival after relapse (11.7 vs. 6.0 months; P=0.0026), in favor of S-1 treatment. However, the researchers point out that in the S-1 group, survival was significantly prolonged in patients with local recurrences and not in other types of relapse (median overall survival: 26.9 vs. 17.8 months; P=0.046). Since there was no increased toxicity with the use of S-1, it is concluded that it is a safe and efficient therapeutic option for patients with gemcitabine-refractory pancreatic adenocarcinoma.
Capecitabine-Lapatinib
He et al. (Abstract #e14542) [31] describe a new open label single-arm phase II study that examines the use of the capecitabine-lapatinib doublet in the second-line therapy of pancreatic adenocarcinoma. Inclusion criteria are an adequate performance status (PS: 0-2), normal hepatic and renal function and failure after gemcitabine-based treatment. Patients will be administered lapatinib on a daily basis and capecitabine for the first two weeks of three-week cycles. In order to achieve a 90% power of statistical significance, the target is to enroll 51 patients over a period of 2 years. The study’s primary endpoint is median overall survival, while microRNA is also analyzed to examine its association with outcome. Since September 2009, 17 patients have been accrued and preliminary results suggest that the regimen is active and of tolerable toxicity.
Discussion
To date, there is no established second-line treatment for patients who exhibit disease progression after gemcitabine-based treatment. Since pancreatic cancer progresses rapidly, patients are often of poor performance status after first-line treatment. Thus, maintaining quality of life is of utmost importance and should be seriously taken into account before proceeding to second-line of treatment. In an effort to address this subject, Kim et al. [32] tried to develop a prognostic model to identify patients who would benefit from second-line treatment. After retrospectively analyzing 90 patients, the researchers concluded that good performance status (PS: 0-1), response to first-line treatment and albumin levels of 3.5 mg/dL or greater were factors that could be used to select cases where second-line therapy would be beneficial.
To our knowledge, up to now, the largest studies evaluating S-1 monotherapy in the second-line setting were one retrospective study by Todaka et al. [19] and two phase II trials (Morizane et al. [20], Sudo et al. [21]). The recent results of the Ishido et al. [30] trial, reported at the 2011 ASCO Annual Meeting, show greater efficacy of S-1 as compared to the three previous studies. More specifically, in the Todaka et al. [19], Morizane et al. [20], and Sudo et al. [21] trials, progression-free survival reached 2.1 months, 2.0 months, and 4.1 months, respectively, while overall survival was reported as 5.8 months, 4.5 months, and 6.3 months, respectively. These reports differ significantly from the data presented in the Ishido et al. trial [30]: survival after relapse was 11.7 months with S-1 and overall survival was 20.9 months. These differences are probably attributed to the fact that patients of the Ishido et al. [30] trial had initially been diagnosed at resectable stage and had undergone surgery, as opposed to patients of the older trials who were diagnosed at advanced stages. It is important to note that patients’ performance status and disease control rates are not stated by Ishido et al. [30] and that the benefit in survival with S-1 was seen in patients with local recurrence and not other recurrence types. Based on the above, it is suggested that S-1 may be beneficial after gemcitabine-failure in certain subgroups of patients.
The combination of capecitabine with a tyrosine kinase (TKI) inhibitor has been studied in the past in the second-line setting after gemcitabine failure. Kulke et al. [29] administered capecitabine plus erlotinib to 30 patients and reported median survival of 6.5 months, with no apparent correlation between response and EGFR mutation status. As erlotinib has been shown to be active in the first-line treatment of pancreatic cancer, there has been growing interest in other growth factor TKIs, such as lapatinib, as well. Lapatinib is a dual TKI inhibitor of human epidermal growth factor receptor 2 (HER2) and epidermal growth factor receptor (EGFR) and since multiple HER pathways are often abnormal in pancreatic adenocarcinoma, lapatinib is expected to be more effective than a single EGFR inhibitor [33]. Regarding the He et al. study design [31], it is notable that patients of performance status equal to 2 are included, which will make this study very informative, since a great percentage of patients are of poor clinical status after gemcitabine failure. We should note that the lapatinib-capecitabine combination was most recently evaluated in the first-line treatment of metastatic pancreatic cancer with poor results, with no objective responses [34]. This could suggest inadequate efficacy of this doublet in the second-line setting as well but the initial results of the He et al. trial [31] show otherwise; therefore, the final results are awaited with great interest. Furthermore, it remains to be seen whether the trial reaches the goal of enrolling 51 patients over a period of 2 years, since only 17 patients have been accrued since September 2009.
In conclusion, despite advances in oncology research, the subject of selecting a second-line regimen after gemcitabine-failure remains controversial. Prospective randomized trials are expected to elucidate the role of novel agents and treatment combinations in selected patients with attention to toxicity.
Conflict of interest
None
References
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61:69-90.
- Oberstein PE, Saif MW. First-line treatment for advanced pancreatic cancer. Highlights from the "2011 ASCO Gastrointestinal Cancers Symposium". San Francisco, CA, USA. January 20-22,2011. JOP. J Pancreas (Online) 2011; 12:96-100.
- Makrilia N, Syrigos KN, Saif MW. Treatment for refractory pancreatic cancer. Highlights from the "2011 ASCO Gastrointestinal Cancers Symposium". San Francisco, CA, USA. January 20-22,2011. JOP. J Pancreas (Online) 2011; 12:110-3.
- Oettle H, Pelzer U., Stieler J., Hilbig A., Roll L., Schwaner I., etal. Oxaliplatin/folinic acid/5-fluorouracil [24h] (OFF) plus bestsupportive care versus best supportive care alone (BSC) in secondline therapy of gemcitabine-refractory advanced pancreatic cancer (CONKO 003). J Clin Oncol 2005; 23(Suppl. 16):4031.
- Pelzer U., Kubica K., Stieler J., Schwaner I., Heil G., Gorner M.,et al. A randomized trial in patients with gemcitabine refractory pancreatic cancer. Final results of the CONKO 003 study. J Clin Oncol 2008; 26(Suppl.):4508.
- Maeda S, Motoi F, Onogawa T, Morikawa T, Shigeru O, Sakata N, et al. Paclitaxel as second-line chemotherapy in patients with gemcitabine-refractory pancreatic cancer: a retrospective study. Int J Clin Oncol 2011; April 1:[Epub ahead of print].
- Saif MW, Syrigos K, Penney R, Kaley K. Docetaxel second-linetherapy in patients with advanced pancreatic cancer: a retrospective study. Anticancer Res 2010; 30:2905-9.
- Renouf DJ, Tang PA, Major P, Krzyzanowska MK, Dhesy-Thind B, Goffin JR, et al. A phase II study of the halichondrin Banalog eribulinmesylate in gemcitabine refractory advanced pancreatic cancer. Invest New Drugs 2011; April 28:-[Epub ahead ofprint].
- Oh SY, Kim HJ, Kim TH, Lee GW, Kim HG, Jeong CY, et al. Pilot study of irinotecan/oxalipltin (IROX) combination chemotherapy for patients with gemcitabine- and 5-fluorouracilrefractory pancreatic cancer. Invest New Drugs 2010; 28:343-9.
- Yoo C, Hwang JY, Kim JE, Kim TW, Lee JS, Park DH, et al. Arandomised phase II study of modified FOLFIRI.3 vs. modified FOLFOX as second-line therapy in patients with gemcitabinere fractory advanced pancreatic cancer. Br J Cancer 2009; 101:1658-63.
- Neuzillet C, Hentic O, Rousseau B, Rebours V, Bengrine-Lefevre L, Raymond E, et al. FOLFIRI regimen as second-/third-line Chemotherapy in patients with advanced pancreatic adenocarcinomarefractory to gemcitabine and platinum salts: A retrospective seriesof 70 patients. 2011 Gastrointestinal Cancers Symposium. J Clin Oncol 2011; 29(Suppl. 4):272.
- Ko AH, Tempero MA, Shan Y, Su W, Lin Y, Dito E, et al. Amultinational phase II study of liposome irinotecan (PEP02) for patients with gemcitabine-refractory metastatic pancreatic cancer.2011 Gastrointestinal Cancers Symposium. J Clin Oncol 2011;29(Suppl. 4):237.
- Boeck S, Wilkowski R, Bruns CJ, Issels RD, Schulz C, Moosmann N, et al. Oral capecitabine in gemcitabine-pretreated patients with advanced pancreatic cancer. Oncology 2007; 73:221-7.
- Saif MW, Kang SP, Ledbetter L, Steg A, Diasio R, Johnson M.Long-term survival on capecitabine in two gemcitabine refractory pancreatic cancer patients. Is there a pharmacogenetic explanation?JOP. J Pancreas (Online) 2007; 8:799-805.
- Fogelman D, Jafari M, Varadhachary GR, Xiong H, Bullock S,Ozer H, et al. Bevacizumab plus gemcitabine and oxaliplatin as firstlinetherapy for metastatic or locally advanced pancreatic cancer: aphase II trial. Cancer Chemother Pharmacol 2011; April 9:-[Epubahead of print].
- Boeck S, Hoehler T, Seipelt G, Mahlberg R, Wein A, Hochhaus A, et al. Capecitabine plus oxaliplatin (CapOx) versus capecitabineplus gemcitabine (CapGem) versus gemcitabine plus oxaliplatin (mGemOx): final results of a multicenter randomized phase II trial inadvanced pancreatic cancer. Ann Oncol 2008; 19:340-7.
- Pino MS, Milella M, Gelibter A, Sperduti I, De MS, Nuzzo C, etal. Capecitabine and celecoxib as second-line treatment of advanced pancreatic and biliary tract cancers. Oncology 2009; 76:254-61.
- Katopodis O, Polyzos A, Kentepozidis N, Giassas S, Rovithi M, Bozionelou V, et al. Second-line chemotherapy with capecitabine (Xeloda) and docetaxel (Taxotere) in previously treated, unresectable adenocarcinoma of pancreas: the final results of a phase II trial.Cancer Chemother Pharmacol 2011; 67:361-8.
- Todaka A, Fukutomi A, Boku N, Onozawa Y, Hironaka S, YasuiH, et al. S-1 monotherapy as second-line treatment for advanced pancreatic cancer after gemcitabine failure. Jpn J Clin Oncol 2010;40:567-72.
- Morizane C, Okusaka T, Furuse J, Ishii H, Ueno H, Ikeda M, etal. A phase II study of S-1 in gemcitabine-refractory metastatic pancreatic cancer. Cancer Chemother Pharmacol 2009; 63:313-9.
- Sudo K, Yamaguchi T, Nakamura K, Denda T, Hara T, IshiharaT, Yokosuka O. Phase II study of S-1 in patients with gemcitabineresistant 2011; 67:249-54.
- Shitara K, Komatsu Y, Yuki S, Munakata M, Muto O, ShimayaS, Sakata Y. Pilot study of combination chemotherapy usingirinotecan plus S-1 for metastatic pancreatic cancer. Oncology 2008;75:67-70.
- Togawa A, Yoshitomi H, Ito H, Kimura F, Shimizu H, Ohtsuka M, et al. Treatment with an oral fluoropyrimidine, S-1, plus cisplatinin patients who failed postoperative gemcitabine treatment for pancreatic cancer: a pilot study. Int J Clin Oncol 2007; 12:268-73.
- O'Reilly EM, Niedzwiecki D, Hall M, Hollis D, Bekaii-Saab T,Pluard T, et al. A Cancer and Leukemia Group B phase II study ofsunitinib malate in patients with previously treated metastatic pancreatic adenocarcinoma (CALGB 80603). Oncologist 2010;15:1310-9.
- Wolpin BM, Hezel AF, Abrams T, Blaszkowsky LS, Meyerhardt JA, Chan JA, et al. Oral mTOR inhibitor everolimus inpatients with gemcitabine-refractory metastatic pancreatic cancer. J Clin Oncol 2009; 27:193-8.
- Astsaturov IA, Meropol NJ, Alpaugh RK, Burtness BA, Cheng JD, Mc Laughlin S, et al. Phase II and Coagulation CascadeBiomarker Study of Bevacizumab With or Without Docetaxel inPatients With Previously Treated Metastatic Pancreatic Adenocarcinoma. Am J Clin Oncol 2011; 34:70-5.
- Ko AH, Venook AP, Bergsland EK, Kelley RK, Korn WM, DitoE, et al. A phase II study of bevacizumab plus erlotinib forgemcitabine-refractory metastatic pancreatic cancer. Cancer Chemother Pharmacol 2010; 66:1051-7.
- Komoto M, Nakata B, Nishii T, Kawajiri H, Shinto O, Amano R, et al. In vitro and in vivo evidence that a combination of lapatinibplus S-1 is a promising treatment for pancreatic cancer. Cancer Sci2010; 101:468-73.
- Kulke MH, Blaszkowsky LS, Ryan DP, Clark JW, Meyerhardt JA, Zhu AX, et al. Capecitabine plus erlotinib in gemcitabinere fractory advanced pancreatic cancer. J Clin Oncol 2007; 25:4787-92.
- Ishido K, Toyoki Y, Kudo D, Nrumi S, Hakamada K. Impact of S-1 as the second-line chemotherapy for patients with relapsing pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):e14588.
- He RR, Hwang JJ, Marshall JJ, Pishvaian M, Slack R, Weiner M, Wellstein A. A phase II study of lapatinib and capecitabine insecond line treatment of locally advanced/metastatic pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):e14542.
- Kim ST, Choi YJ, Park KH, Oh SC, Seo JH, Shin SW, et al. APrognostic Model to Identify Patients with Advanced Pancreas Adenocarcinoma Who Could Benefit from Second-line Chemotherapy. Clin Oncol (R Coll Radiol ) 2011; March 5:-[Epubahead of print].
- Safran H, Miner T, Resnick M, Dipetrillo T, Mc Nulty B, Evans D, et al. Lapatinib/gemcitabine and lapatinib/gemcitabine/oxaliplatin:a phase I study for advanced pancreaticobiliary cancer. Am J Clin Oncol 2008; 31:140-4.
- McDermott RS, Calvvert P, Parker M, Webb G, Moulton B, Mc Caffrey J, Irish Clinical Oncology Research Group. A phase IIstudy of lapatinib and capecitabine in first-line treatment of metastatic pancreatic cancer (ICORG 08-39). J Clin Oncol 2011;29(Suppl. 4):315.
- Saif MW. Pancreatic cancer: are we moving forward yet?Highlights from the Gastrointestinal Cancers Symposium. Orlando,FL, USA. January 20th, 2007. JOP. J Pancreas (Online) 2007; 8:166-76.


