Keywords
Carcinoma; Drug Therapy; gemcitabine; Neoplasm Metastasis; Pancreas; Pancreatic Neoplasms; Therapeutics
Abbreviations
FOLFIRINOX: combination of 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin; SPARC: secreted protein acidic and rich in cysteine
On September 6th, 2013, the U.S. Food and Drug Administration (FDA) approved paclitaxel proteinbound particles (albumin-bound) (Abraxane® for injectable suspension, Abraxis BioScience, LLC, a wholly owned subsidiary of Celgene Co., Summit, NJ, USA), in combination with gemcitabine for the firstline treatment of patients with metastatic adenocarcinoma of the pancreas based on the MPACT study which demonstrated a clinically meaningful increase in overall survival [1].
The promising results of a phase I/II study led to the performance of this phase III study named MPACT [2]. MPACT was a multi-center, international, open-label, randomized trial that enrolled 861 patients with metastatic pancreatic cancer. Patients were randomized to receive either the combination of Abraxane® plus gemcitabine (n=431) or gemcitabine alone (n=430). Randomization was stratified by geographic region (Australia, Western Europe, Eastern Europe, or North America), performance status, and presence of liver metastasis. The primary endpoint was overall survival (OS) and secondary objectives included progression-free survival (PFS) and overall response rate (ORR), both assessed by independent, central, blinded radiological review using Response Evaluation Criteria In Solid Tumors (RECIST) criteria (version 1.0) [3].
The demographic characteristics were wellbalanced between the arms. The median age of the patients was 63 years (range: 27-88 years) with 42% aged 65-years or older, 58% were men, and the Karnofsky performance was 90 or 100 in 60%. Nearly half (46%) of the patients had three or more sites of metastatic disease and 84% had liver metastases. The primary lesion was located in the pancreatic head in 43%, the body in 31%, or tail in 25% of patients. The results are summarized in Table 1.
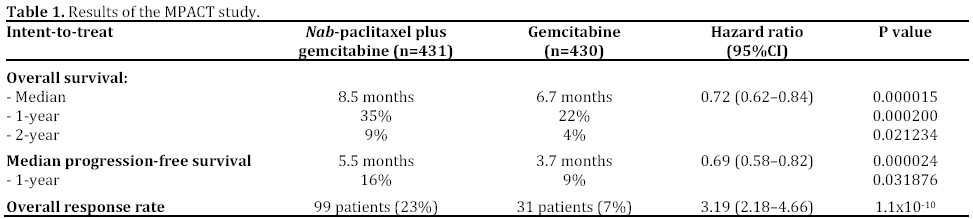
Grade ≥3 adverse events were more common in the combination arm compared to single agent gemcitabine and included neutropenia (38% vs. 27%), fatigue (17% vs. 7%), and neuropathy (17% vs. 1%). However, the grade ≥3 neuropathy improved to grade1 or less within 29 days.
The recommended dose and schedule for Abraxane® is 125 mg/m2 administered as an intravenous infusion over 30-40 minutes on days 1, 8 and 15 of each 28-day cycle until disease progression or if no longer tolerated by the patient. Gemcitabine is administered immediately after Abraxane® on days 1, 8 and 15 of each 28-day cycle. Full prescribing information is available in the FDA web-site [4].
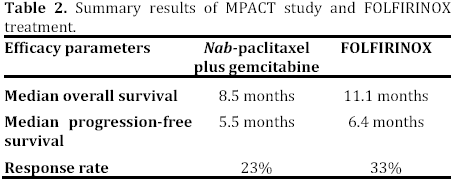
This regimen now offers a new option for first line treatment of advanced pancreatic cancer. Nabpaclitaxel has already been approved to treat advanced breast cancer and non-small-cell lung cancer. A non-gemcitabine regimen, FOLFIRINOX (combination of 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin) has already emerged recently and adopted by many oncologists worldwide [5]. A number of factors influence which drug combination that clinicians will chose in the future. One can question that the median survival with nab-paclitaxel plus gemcitabine (8.5 months) is almost three months less than that of FOLFIRINOX (Table 2). However, it is difficult to draw any conclusions since these two regimens were not compared directly in the same trial.
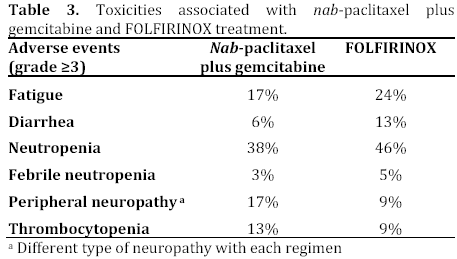
Both studies have well-balanced demographic characteristics and none of those features seem to help us identifying the right patient for an individual regimen. The toxicities are different (Table 3) for these two regimens. Toxicity has been a concern with the 4-drug combination. While the overall survival of patients treated with gemcitabine and Abraxane® does not reach the level seen in patients treated with FOLFIRINOX, the toxicity profile of this combination seems more favorable, especially with respect to neutropenia and fatigue.
Another important factor to consider is the financial burden. The New York Times reported that nabpaclitaxel will cost $6,000 to $8,000 a month for a pancreatic cancer patients, a cost likely to be more expensive than FOLFIRINOX [6]. On the other hand, FOLFIRINOX is a toxic regimen if given in full doses and requires the patient to wear an infusion pump for 5-fluorouracil. It is my expectation that both regimens will be used by the physicians in selected patients and their preferences. FOLFIRINOX may be best used in younger patients younger with a good performance status.
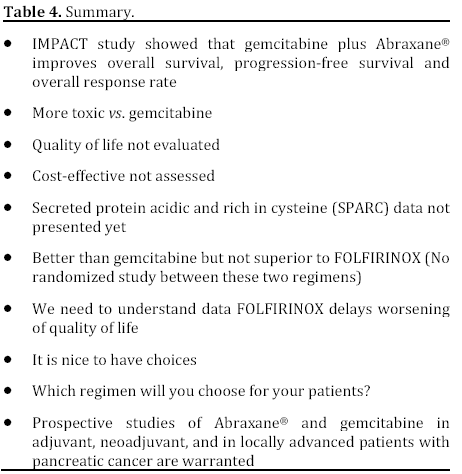
There is a need to identify which patients will ultimately benefit from one of these regimens (Table 4). The correlation between secreted protein acidic and rich in cysteine (SPARC) expression and outcome is pending on MPACT study.
Conflict of interest
The author has no potential conflicts of interest
References
- Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood TE, et al. Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: a phase I/II trial. J Clin Oncol 2011; 29:4548-54. [PMID 21969517]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; Oct 16. [PMID 24131140]
- Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000; 92:205-16. [PMID 10655437]
- U.S. Food and Drug Administration. FDA approved drug products: Abraxane. Label Information. September 6th, 2013.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-25. [PMID 21561347]
- Pollack A. Drug is shown to help pancreatic cancer cases. The New York Time 2013; January 22. (Last accessed on October 26, 2013)

