Abbreviations
DPPHR: duodenum-preserving pancreatic head resection
INTRODUCTION
Chronic pancreatitis is characterised by recurrent abdominal pain and progressive destruction of pancreatic parenchyma leading to exocrine and endocrine deficiency [1, 2, 3]. The spectrum of disease is variable and ranges from mild attacks to severe debilitating disease. The incidence of chronic pancreatitis is not well characterised but a French study reports figures in the order of 5-10 cases per 100,000 population [4]. The pathological changes within the pancreas vary and include dilatation of the main pancreatic duct (either uniformly or in a characteristic segmental form), parenchymal calcification and cystic change. These changes can either be localised or diffusely spread throughout the gland [1].
Surgical treatment for chronic pancreatitis has been reported to provide good relief of symptoms [5, 6]. Types of abdominal surgical intervention for chronic pancreatitis can be broadly categorised into pancreatic resectional procedures or drainage operations. Newer operations include minimally invasive division of the splanchnic nerves in the thoracic cavity [7]. However, the evidence to guide the selection of any given intervention is limited. In particular, reporting of baseline clinical assessment data are limited and thus patients in different centres may be presenting and undergoing surgery at different stages of their illness. Also, the information to guide selection between resection and drainage is limited and a number of centres appear to promote an operation or procedure developed within their particular unit. This study undertakes a systematic overview of elective surgery for chronic pancreatitis with particular reference to assessment of indication for surgery, type of surgery employed and relation between indication and type of surgery.
PATIENTS AND METHODS
A computerised search of the PubMed, Embase and Cochrane databases was performed using the search engine ADITUS for the period from June 1997 to June 2007. The Medical Subject Headings (MeSH) “Chronic pancreatitis” and “Surgery” were used. The results were combined using Boolean operators to yield a total of 374 articles. Only articles providing original information were retained. Articles which were reviews, case reports, referred to patients with known pancreatic malignancy or which did not providing original information were excluded. In cases of sequential publication of data, the manuscript providing the most detail was retained. These exclusions produced a final study population of 46 manuscripts providing data on 4,626 patients undergoing elective surgery for chronic pancreatitis. The manuscripts were then reviewed and data extracted on demographic profile including aetiology of chronic pancreatitis, gender, country of publication and study period. Specific information was then sought on whether chronic pancreatitis was defined in the manuscript, whether information was provided on the indication for surgery, whether quality of life assessments were undertaken and on the type of surgery undertaken with particular reference to whether information was provided on the relationship between the indication for surgery and the type of surgery undertaken. Data on outcome of surgery were also sought. All manuscripts were reviewed independently by two authors and a final agreed dataset utilised for analysis.
STATISTICS
Two by two tables are analysed by Fisher’s exact and the Mann-Whitney U tests using the Statsdirect software package (version 2.6.5., www.statsdirect.com).
RESULTS
Demographic Profile
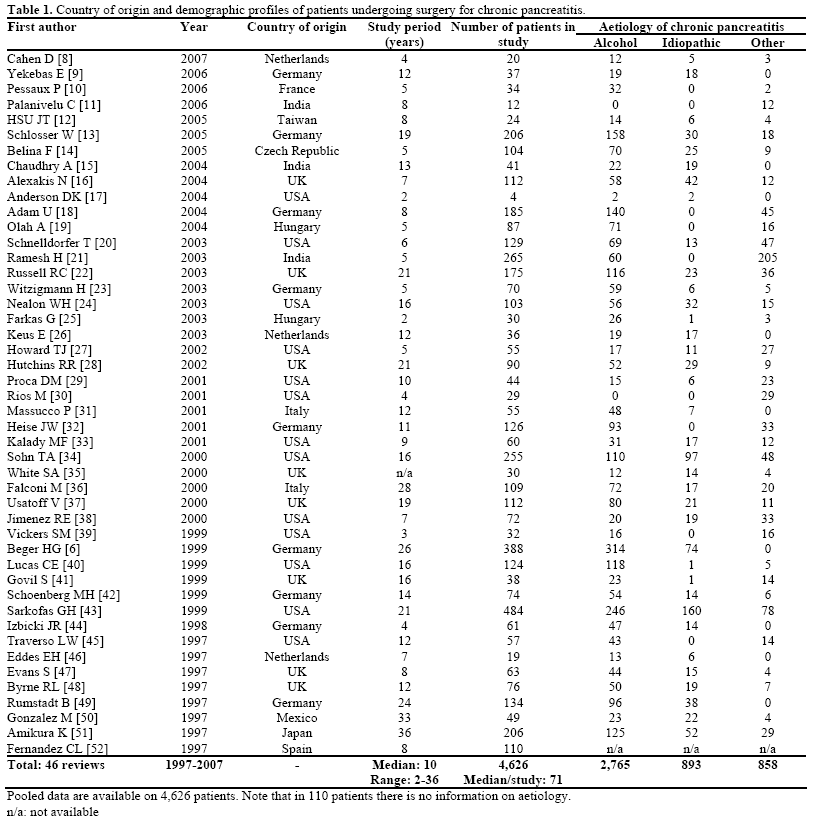
The study population comprised 4,626 patients reported in 46 studies [8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52]. The median number of patients per study was 71 (range 4-484) (Table 1). Twenty six (56.5%) reports originated from Europe, 14 (30.4%) from the United States of America, 5 (10.9%) from Asia/Far-East and 1 (2.2%) from Mexico. The median study period for recruitment (including follow-up) of patients was 10 years (range: 2-36 years). There were 3,337 (72.1%) males. The most common aetiology was alcohol in 2,765 (61.2%) patients (note that aetiology was not available for 110 patients). Other aetiologies included idiopathic chronic pancreatitis in 893 (19.8%), tropical chronic pancreatitis in 209 (4.6%) and “others” in 649 (14.4%).
Description of Indications for Surgery
We found one only study without indications (Olah A, et al. [19]); therefore, the indication for surgery was described in 45 of 46 articles (97.8%) for a total of 4,539 patients. Of the listed indications, abdominal pain was the principal factor in 3,833 (84.4%) patients (Table 2). Formal comparison of pre-operative and post-operative pain scores was provided in 15 manuscripts (32.6%) (Table 3). Similarly, pre and postoperative analgesic usage was reported in 18 (39.1%).


Type of Surgery
Pancreatic head resectional surgery (either conventional Whipple or pylorus-preserving variant) was the most frequently undertaken procedure in this series being undertaken in 1,206 (26.1%) (Table 2). Duodenum-preserving pancreatic head resection (DPPHR) was undertaken in 745 (16.1%). Distal pancreatectomy (with or without splenic preservation) was undertaken in 563 (12.2%). Total pancreatectomy (with or without spleen and duodenum preservation) was undertaken in 122 (2.6%). Of drainage procedures, lateral pancreatico-jejunostomy was the most frequently reported being described in 989 (21.4%). In terms of the distribution of procedures across centres, the number of services reporting the use of DPPHR was13, of which 4 services reported a combined total of 16 patients undergoing DPPHR. The number of centres reporting the use of the V-shaped excision of pancreatic head was 1 (in 37 patients). Only seven (15%) reports provide a formal rationale or indication for selection of the type of elective surgical procedure for a stated disease variant and these papers cover 481 (10.4%) patients.
Operative Outcome
There were 179 (3.9%) in-hospital deaths after surgery. One thousand and seventy five (23.2%) patients had one or more surgical complications. Thirty eight (82.6%) reports gave information on a total of 1,609 (39.7%) patients with post-operative diabetes from a total population of 4,056 patients in these reports. Prior to surgery, 908 (22.0%) of 4,129 patients were reported to have diabetes mellitus. After surgery (interval not consistently reported), 1,609 (39.7%) of 4,056 were diabetic and this difference was significant (P<0.001; Fisher’s exact test).
Pain Assessment
Fifteen studies provided data on pain scores before and after surgery (Table 3). Comparison of pooled preoperative pain scores to those after surgery (accepting the variable median follow-up) shows a significant reduction in pain (P<0.002; Mann-Whitney U test).
Use of Quality of Life Assessments
An externally validated quality of life questionnaire such as either the short form 36 (SF-36) or the European Organisation for Research and Treatment of Cancer’s quality of life questionnaire with pancreasspecific module (EORTC QLQ C-30 plus PAN-26) [53] is reported in 8 (17.3%) of 46 manuscripts covering 441 (9.5%) of 4,626 patients (Table 2). Seven of these studies reported quality of life assessment comparing pre and post operative values. In addition, 5 studies have described the outcome/quality of life using non-validated questionnaire.
DISCUSSION
This article has undertaken a systematic overview of reports on elective surgery for chronic pancreatitis. With 4,626 patients undergoing elective surgery included in the study population of 46 reports, this is one of the largest patient cohorts reported. It is accepted that despite stringent computerised database searches and the precaution of cross-checking databases it is likely that not all relevant articles will have been captured and that there will be a bias toward publication of manuscripts with “positive” results. Nevertheless, the study population is thought to be representative of surgical practice in chronic pancreatitis. Other important methodological limitations are likely to include variation in definition of chronic pancreatitis, differences in case selection and probably differences in interpretation of the exact nature of a specific surgical procedure (such as the DPPHR) between reports. However, interpretation of the data presented here while keeping these limitations in mind has highlighted several interesting and consistent trends across reports
First, our study shows that almost twice as many reports originate from Europe as compared to the United States of America (Table 1). The reason for this difference is not apparent from these studies and may be multifactorial but could also reflect differences in clinical practice rather than true differences in disease incidence.
Second, it can be seen that median recruitment time to these studies is lengthy (Table 1), suggesting that even in specialist units, relatively few patients are submitted to surgery. In turn, this may mean that individual units are less able to sustain randomized comparative trials and also that collective experience of the surgical management of chronic pancreatitis may be relatively limited.
The findings that alcohol was the most frequent etiologic agent and pain the most often quoted indication for surgery are not new.
Although “pain and complications” were the most frequently cited indications for surgery (Table 2), the relative dearth of use of pre-operative pain scores or quality of life assessments could be regarded as a critical limitation of the published literature. It is difficult to compare between reports (in particular reports recommending different procedures for chronic pancreatitis) when it is not certain whether all reports are referring to the same baseline disease burden or pain levels. Similarly, it is not possible from the wide variety of operative interventions undertaken in patients with “pain and complications” to match type of surgical intervention to disease presentation. It could be further argued that the wide variation in duration of disease interval prior to surgery (Table 2) is indirect evidence that centres are reporting operative interventions on patients at different disease stages.
Although all reports refer to elective surgery in patients with chronic pancreatitis, some operative procedures are carried out for the complications of chronic pancreatitis rather than undertaking resection or drainage of the diseased gland and hence the range of reported interventions include pseudocyst drainages (Table 2).
In a chronic and essentially stable although disabling condition, it was a surprising finding to report that so few studies undertook formal quality of life assessment. One explanation could be that questionnaires validated for use in chronic pancreatitis have only recently become widely available. However, over a decade ago, Izbicki’s group were using quality of life assessment questionnaires to assess the outcome of surgery [44].
In terms of the type of surgery undertaken, although the Whipple-type pancreatic head resection was the most frequently undertaken, it appears that a contemporary trend is more towards duodenumpreserving pancreatic head resection. Of particular interest is the limited information provided in terms of matching of operative procedure to disease variant. Further, it appears that particular units undertake procedures developed within those units.
Currently available pointers for selection of treatment option include head resection by pancreaticoduodenectomy where there may be concerns about underlying malignancy and drainage in patients with duct dilatation in the absence of a pancreatic head mass. However, the treatment of patients with small duct disease remains unclear and in our study, patients with this type of disease were treated by the Izbicki operation by one group [9] but by other procedures by others [21, 43]. Similarly, criteria for case selection for duodenum preserving head resection compared to pancreaticoduodenectomy are unclear. A rational allocation of role in this management algorithm for thoracoscopic splanchnic nerve division is also required
It is encouraging to note that there is more recent published evidence providing long-term outcome data on a randomized trial comparing Whipple pancreaticoduodenectomy to duodenum-preserving pancreatic head resection [54].
In conclusion, this study demonstrates that there remains a pressing lack of standardization between units in relation to the criteria for operative intervention in painful chronic pancreatitis. In a vulnerable patient group and in the setting of an essentially stable disease, this lack of concordance is clearly highlighted in this overview and is difficult to justify in contemporary surgical practice. From our findings, it would seem logical to suggest that if clinicians are to undertake surgery for chronic pancreatitis that at a minimum, formal quality of life testing using a validated system is undertaken in all patients prior to elective surgery for painful chronic pancreatitis. In addition, longer-term follow-up is required before reporting of data.
Conflicts of interest
None
Acknowledgement
Papers based on this manuscript were read at the 8th World Congress of the International Hepato-Pancreato-Biliary Association, Mumbai, India, 29th February 2008 and appeared in abstract form (HPB 2008; 10: Suppl 1) and also as a poster at the American Hepato-Pancreato-Biliary Association, Fort Lauderdale, USA, March 2008 (HPB 2008; 10: Suppl 2).
References
- Singer MV, Gyr K, Sarles H. Revised classification of pancreatitis. Report of the Second International Symposium on the Classification of Pancreatitis in Marseille, France, March 28-30, 1984. Gastroenterology 1985; 89:683-5. [PMID 4018507]
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128:586-90. [PMID 8489394]
- Lankisch PG, Löhr-Happe A, Otto J, Creutzfeldt W. Natural course in chronic pancreatitis. Pain, exocrine and endocrine pancreatic insufficiency and prognosis of the disease. Digestion 1993; 54:148-55. [PMID 8359556]
- Lévy P, Barthet M, Mollard BR, Amouretti M, Marion-Audibert AM, Dyard F. Estimation of the prevalence and incidence of chronic pancreatitis and its complications. Gastroenterol Clin Biol 2006; 30:838-44. [PMID 16885867]
- Schlosser W, Poch B, Beger HG. Duodenum-preserving pancreatic head resection leads to relief of common bile duct stenosis. Am J Surg 2002; 183:37 41. [PMID 11869700]
- Beger HG, Schlosser W, Friess HM, Büchler MW. Duodenumpreserving head resection in chronic pancreatitis changes the natural course of the disease: a single-center 26-year experience. Ann Surg 1999; 230:512-9. [PMID 10522721]
- Hammmond B, Vitale GC, Rangnekar N, Vitale EA, Binford JC. Bilateral thoracoscopic splanchnicectomy for pain control in chronic pancreatitis. Am Surg 2004; 70:546-9. [PMID 15212413]
- Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med 2007; 15;356:676-84. [PMID 17301298]
- Yekebas EF, Bogoevski D, Honarpisheh H, Cataldegirmen G, Habermann CR, Seewald S, et al. Long-term follow-up in small duct chronic pancreatitis: A plea for extended drainage by "V-shaped excision" of the anterior aspect of the pancreas. Ann Surg 2006; 244:940-6; discussion 946-8. [PMID 17122619]
- Pessaux P, Kianmanesh R, Regimbeau JM, Sastre B, Delcenserie R, Sielezneff I, et al. Frey procedure in the treatment of chronic pancreatitis: short-term results. Pancreas 2006; 33:354-8. [PMID 17079939]
- Palanivelu C, Shetty R, Jani K, Rajan PS, Sendhilkumar K, Parthasarthi R, Malladi V. Laparoscopic lateral pancreaticojejunostomy: a new remedy for an old ailment. Surg Endosc 2006; 20:458-61. [PMID 16424983]
- Hsu JT, Yeh CN, Hwang TL, Chen HM, Jan YY, Chen MF. Outcome of pancreaticoduodenectomy for chronic pancreatitis. J Formos Med Assoc 2005; 104:811-5. [PMID 16496060]
- Schlosser W, Siech M, Beger HG. Pseudocyst treatment in chronic pancreatitis--surgical treatment of the underlying disease increases the long-term success. Dig Surg 2005; 22:340-5. [PMID 16293964]
- Belina F, Fronek J, Ryska M. Duodenopancreatectomy versus duodenum-preserving pancreatic head excision for chronic pancreatitis. Pancreatology 2005; 5:547-52. [PMID 16110253]
- Chaudhary A, Negi SS, Masood S, Thombare M. Complications after Frey's procedure for chronic pancreatitis. Am J Surg 2004; 188:277-81. [PMID 15450834]
- Alexakis N, Sutton R, Raraty M, Connor S, Ghaneh P, Hughes ML, et al. Major resection for chronic pancreatitis in patients with vascular involvement is associated with increased postoperative mortality. Br J Surg 2004; 91:1020-6. [PMID 15286965]
- Andersen DK. Topazian MD. Pancreatic head excavation: a variation on the theme of duodenum-preserving pancreatic head resection. Arch Surg 2004; 139:375-9. [PMID 15078703]
- Adam U, Makowiec F, Reidiger H, Keck T, Kroger JC, Uhrmeister P, Hopt TU. Pancreatic head resection for chronic pancreatitis in patients with extrahepatic generalized portal hypertension. Surgery 2004; 135:411-8. [PMID 15041965]
- Oláh A, Kelemen D, Horvath OP, Belágyi T. Long-term followup results of surgery for chronic pancreatitis. Hepatogastroenterology 2004; 5:1179-82. [PMID 15239273]
- Schnelldoreer T, Adams DB. Outcome after lateral pancreaticojejunostomy in patients with chronic pancreatitis associated with pancreas divisum. Am Surg 2003; 69:1041-4. [PMID 14700288]
- Ramesh H, Jacob G, Lekha V, Venugopal A. Ductal drainage with head coring in chronic pancreatitis with small-duct disease. J Hepatobiliary Pancreat Surg 2003; 10:366-72. [PMID 14598137]
- Russell RC, Theis GN. Pancreatoduodenectomy in the treatment of chronic pancreatitis. World J Surg 2003; 27:1203-10. [PMID 14534820]
- Witzigmann H, Max D, Uhlmann D, Geissler F, Schwarz R, Ludwig S, et al. Outcome after duodenum-preserving pancreatic head resection is improved compared with classic Whipple procedure in the treatment of chronic pancreatitis. Surgery 2003; 134:53-62. [PMID 12874583]
- Nealon WH, Walser E. Duct drainage alone is sufficient in the operative management of pancreatic pseudocyst in patients with chronic pancreatitis. Ann Surg 2003; 237:614-20; discussion 620-2. [PMID 12724627]
- Farkas G, Leindler L, Daróczi M, Farkas G Jr. Organ-preserving pancreatic head resection in chronic pancreatitis. Br J Surg 2003; 90:29-32. [PMID 12520571]
- Keus E, van Laarhoven CJ, Eddes EH, Masclee AA, Schipper ME, Gooszen HG. Size of the pancreatic head as a prognostic factor for the outcome of Beger's procedure for painful chronic pancreatitis. Br J Surg 2003; 90:320-4. [PMID 12594667]
- Howard TJ, Swofford JB, Wagner DL, Sherman S, Lehman GA. Quality of life after bilateral thoracoscopic splanchnicectomy: longterm evaluation in patients with chronic pancreatitis. J Gastrointest Surg 2002; 6:845-52. [PMID 12504223]
- Hutchins RR, Hart RS, Pacifico M, Bradley NJ, Williamson RC. Long-term results of distal pancreatectomy for chronic pancreatitis in 90 patients. Ann Surg 2002; 236:612-8. [PMID 12409667]
- Proca DM, Ellison EC, Hibbert D, Frankel WL. Major pancreatic resections for chronic pancreatitis. Arch Pathol Lab Med 2001; 125:1051-4. [PMID 11473456]
- Rios GA, Adams DB. Outcome of surgical treatment of chronic pancreatitis associated with sphincter of Oddi dysfunction. Am Surg 2001; 67:462-6. [PMID 11379650]
- Massucco P, Calgaro M, Bertolino F, Bima C, Galatola G, Capussotti L. Outcome of surgical treatment for chronic calcifying pancreatitis. Pancreas 2001; 22:378-82. [PMID 11345138]
- Heise JW, Katoh M, Lüthen R, Röher HD. Long-term results following different extent of resection in chronic pancreatitis. Hepatogastroenterology 2001; 48:864-8. [PMID 11462943]
- Kalady MF, Broome AH, Meyers WC, Pappas TN. Immediate and long-term outcomes after lateral pancreaticojejunostomy for chronic pancreatitis. Am Surg 2001; 67:478-83. [PMID 11379654]
- Sohn TA, Campbell KA, Pitt HA, Sauter PK, Coleman JA, Lillemo KD, et al. Quality of life and long-term survival after surgery for chronic pancreatitis. J Gastrointest Surg 2000; 4:355-64. [PMID 11058853]
- White SA, Sutton CD, Weymss-Holden S, Berry DP, Pollard C, Rees Y, Dennison AR. The feasibility of spleen-preserving pancreatectomy for end-stage chronic pancreatitis. Am J Surg 2000; 179:294-7. [PMID 10875989]
- Falconi M, Valerio A, Caldiron E, Salvia R, Sartori N, Talamini G, et al. Changes in pancreatic resection for chronic pancreatitis over 28 years in a single institution. Br J Surg 2000; 87:428-33. [PMID 10759737]
- Usatoff V, Brancatisano R, Williamson RC. Operative treatment of pseudocysts in patients with chronic pancreatitis. Br J Surg 2000; 87:1494-9. [PMID 11091235]
- Jimenez RE, Fernandez-del Castillo C, Rattner DW, Chang Y, Warshaw AL. Outcome of pancreaticoduodenectomy with pylorus preservation or with antrectomy in the treatment of chronic pancreatitis. Ann Surg 2000; 231:293-300. [PMID 10714621]
- Vickers SM, Chan C, Heslin MJ, Bartolucci A, Aldrete JS. The role of pancreaticoduodenectomy in the treatment of severe chronic pancreatitis. Am Surg 1999; 65:1108-11. [PMID 10597055]
- Lucas CE, McIntosh B, Paley D, Ledgerwood AM, Vlahos A. Surgical decompression of ductal obstruction in patients with chronic pancreatitis. Surgery 1999; 126:790-5. [PMID 10520930]
- Govil S, Imrie CW. Value of splenic preservation during distal pancreatectomy for chronic pancreatitis. Br J Surg 1999; 86:895-8. [PMID 10417561]
- Schoenberg MH, Schlosser W, Rück W, Beger HG. Distal pancreatectomy in chronic pancreatitis. Dig Surg 1999; 16:130-6. [PMID 10207239]
- Sakorafas GH, Farnell MB, Farley DR, Rowland CM, Sarr MG. Long-term results after surgery for chronic pancreatitis. Int J Pancreatol 2000; 27:131-42. [PMID 10862512]
- Izbicki JR, Bloechle C, Broering DC, Knoefel WT, Kuechler T, Broelsch CE. Extended drainage versus resection in surgery for chronic pancreatitis: a prospective randomized trial comparing the longitudinal pancreaticojejunostomy combined with local pancreatic head excision with the pylorus-preserving pancreatoduodenectomy. Ann Surg 1998; 228:771-9. [PMID 9860476]
- Traverso WL, Kozarek RA. Pancreatoduodenectomy for chronic pancreatitis: anatomic selection criteria and subsequent long-term outcome analysis. Ann Surg 1997; 226:429-35. [PMID 9351711]
- Eddes EH, Masclee AM,Gooszen HG, Frolich M, Lamers CB. Effect of duodenum-preserving resection of the head of the pancreas on endocrine and exocrine pancreatic function in patients with chronic pancreatitis. Am J Surg 1997; 174:387-92. [PMID 9337159]
- Evans JD, Wilson PG, Carver C, Bramhall SR, Buckels JA, Mayer AD, et al. Outcome of surgery for chronic pancreatitis. Br J Surg 1997; 84:624-9. [PMID 9171747]
- Byrne RL, Gompertz RH, Venables CW. Surgery for chronic pancreatitis: a review of 12 years experience. Ann R Coll Surg Engl 1997; 79:405-9. [PMID 9422864]
- Rumstadt B, Forssmann K, Singer MV, Trede M. The Whipple partial duodenopancreatectomy for the treatment of chronic pancreatitis. Hepatogastroenterology 1997; 44:1554-9. [PMID 9427021]
- González M, Herrera MF, Laguna M, Gamino R, Uscanga L, Robles-Díaz G, et al. Pain relief in chronic pancreatitis by pancreatico-jejunostomy. An institutional experience. Arch Med Res 1997; 28:387-90. [PMID 9291636]
- Amikura K, Arai K, Kobari M, Matsuno S. Surgery for chronic pancreatitis--extended pancreaticojejunostomy. Hepatogastroenterology 1997; 44:1547-53. [PMID 9427020]
- Fernández-Cruz L, Sabater L, Pera M, Astudillo E, Sáenz A, Navarro S. Conservative pancreatic resection in patients with obstructive chronic pancreatitis. Hepatogastroenterology 1997; 44:1023-8. [PMID 9261593]
- Fitzsimmons D, Kahl S, Butturini G, van Wyk M, Bornman P, Bassi C, et al. Symptoms and quality of life in chronic pancreatitis assessed by structured interview and the EORTC QLQC30 and QLQ-PAN26. Am J Gastroenterol 2005; 100:918-926. [PMID 15784041]
- Muller MW, Friess H,Martin DJ, Hinz U, Dahmen R, Buchler MW. Long-term follow-up of a randomized clinical trial comparing Beger with pylorus-prserving Whipple procedure for chronic pancreatitis. Br J Surg 2008; 95:350-6. [PMID 17933005]

