Keywords
Esophageal and Gastric Varices; Hypertension, Portal; Mesenteric Veins; Pancreatitis; Portal Vein; Splenic Vein
Abbreviations
CP: Chronic Pancreatitis SV Splenic vein PV Portal vein SPH Sinistral portal hypertension SMV Superior mesenteric vein CTPV Cavernous transformation of the portal vein TIPS Transjugular Intrahepatic Portosystemic Shunts PH Portal hypertension PB Portal biliopathy GWV Gallbladder wall varices THAD Transient Hepatic Attenuation Difference EUS Endoscopic ultrasonography
INTRODUCTION
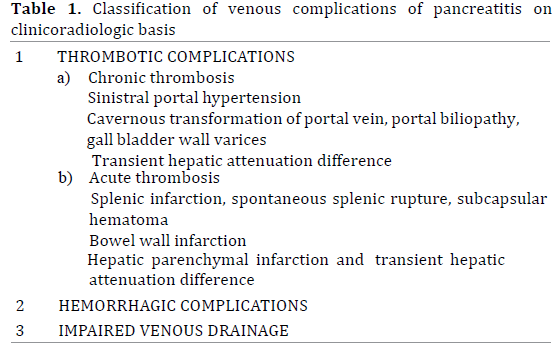
Pancreatitis is a systemic disease owing to release of inflammatory mediators and digestive enzymes. Consequently, pancreatitis associated complications can be myriad with vascular complications being a well known but infrequent phenomenon. These vascular complications are seen in 25% patients suffering from pancreatitis and entail significant morbidity and mortality [1]. There is predominant affliction of peripancreatic arteries. Venous complications are less commonly reported and are often confined to thrombosis of the vein. Isolated case reports and series of unusual but significantly morbid venous complications associated with pancreatitis have, however, been described. This article focuses on multitudinous venous complications in the setting of pancreatitis and classifies the potential venous complications on clinicoradiologic grounds into 3 categories: thrombotic or hemorrhagic complications and complications arising due to impaired venous drainage (table 1).
THROMBOTIC COMPLICATIONS IN PANCREATITIS
Venous thrombosis is the most common complication of pancreatitis affecting venous system. A surge in procoagulant inflammatory mediators, stasis, vessel spasm, mass effects from the surrounding inflamed pancreas causes thrombosis in acute pancreatitis [2] whereas etiology in chronic pancreatitis (CP) includes intimal injury due to repeated acute inflammation, chronic inflammation with fibrosis, compressive effects of a pseudocyst or an enlarged inflamed pancreas [3]. Close anatomic ties with pancreas results in splenic vein involvement in majority of the cases [4]. Prevalence of splenic vein and portal vein thrombosis in CP is 22% (Agrawal et al.) and 5.6% (Bernades et al.), respectively. Attempts to healing cause collateral formation responsible for left-sided hypertension in the former while cavernous transformation of portal vein, portal biliopathy and gall bladder wall varices in the latter.
Chronic Thrombosis of Splenic Vein and Formation of Collaterals
A chronic obstruction to venous return from splenic vein (SV) can give rise to a compartmentalised form of portal hypertension called leftsided or Sinistral Portal Hypertension (SPH) [5]. Etiology of SPH is multifactorial and in cases of pancreatitis includes SV thrombosis [6] or SV compression from mass-forming chronic pancreatitis or a pseudocyst [5, 6]. CP associated SV thrombosis is the most common cause of SPH [6]. It may, however, be difficult to demonstrate the clot or SV itself in CP. Hence, the diagnosis involves detection of collaterals [7] which include the short and posterior gastric and the gastroepiploic collaterals [8]. While the former drain via coronary vein into the portal vein (PV) [8], the latter join the superior mesenteric vein (SMV) [8]. Flow direction is still hepatopetal [7] since primary pathology is not hepatic in origin. Imaging features include signs of pancreatic pathology, splenomegaly, splenic hilar and gastric and or gastroesophageal collaterals with normal portal vein and normal liver morphology [5, 6]. A late-phase celiac angiography may depict an occluded splenic vein.These gastric [5] or gastroesophageal [9] collaterals may manifest as variceal bleed. Upper gastrointestinal hemorrhage in SPH, however, is a rarity and constitutes upto 1% of life threatening upper gastrointestinal bleed [6]. In the series described by Agrawal et al. only 15% of patients with CP associated SV thrombosis presented with hematemesis [10].
More selective and compartmentalized forms of portal hypertension following CP associated SV thrombosis have also been described. Burbige et al. reported a case of chronic pancreatitis with per rectal bleeding. Colonoscopy demonstrated colonic varices at splenic flexure and angiography revealed an occluded SV and hence the collaterals [11]. There is no correlation between the incidence of SPH and the severity of pancreatitis [6]; SPH may be a consequence of a mild or subclinical episode of pancreatitis [6].
It is important to exclude other causes of portal hypertension and liver pathologies [5, 6] since management for SPH is completely different [6]. While variceal clipping or Transjugular Intrahepatic Portosystemic Shunts (TIPS) is the procedure of choice for refractory bleed from collaterals in liver cirrhosis [6], splenectomy with correction of primary pathology i.e., a compressing pseudocyst or CP associated adhesions, is the management of choice in symptomatic SPH [5, 6, 8]. The rationale for splenectomy is decompression of splenic hilar venous collaterals on interruption of arterial supply [8]. Presence of numerous hilar collaterals favour an open surgical approach. [8]. However, Patrono et al. described a successful laparoscopic splenectomy following splenic artery embolization in a symptomatic case of CP associated SV thrombosis. For poor surgical candidates, splenic artery embolization has been described as a viable option [12] wherein the end point of procedure is partial embolization of the artery. Management in asymptomatic SPH is controversial with some authors advising prophylactic splenectomy [6]. Agrawal et al. advocated splenectomy even in asymptomatic patients with CP associated SPH [6, 10]. The authors stated that performing splenectomy did not increase morbidity or mortality [10]. The current evidence however, favors a conservative approach in asymptomatic individuals [6]. Heider et al. studied 53 patients of CP associated SPH and advised against routine splenectomy in these patients [13].
Cavernous Transformation of Portal Vein, Portal Biliopathy and Gall Bladder Wall Varices: Sequelae to Chronic Portal Vein Thrombosis
Cavernous Transformation of Portal Vein
When the thrombus occludes the main PV, the hepatopetal flow is maintained via cavernous transformation of the portal vein (CTPV) (Figure 1)[14]. Besides a lumen occluding thrombus, a pseudocyst or mass-forming chronic pancreatitis may also cause extrinsic compression of the PV and consequently CTPV [4]. CTPV comprises of two sets of veins: the paracholedochal veins of Petren, that run parallel to biliary duct wall and the epicholedochal veins of Saint, that are located on the surface of bile ducts [15]. It takes approximately 3 weeks’ time for cavernous transformation to occur[16]. CTPV is found in 70 -100% of patients suffering from PV thrombosis. In spite of numerous collateral pathways, portal hypertension (PH) still occurs. Patients become symptomatic on account of features of portal hypertension i.e., bleeding from collaterals and splenomegaly than due to biliary obstruction caused by enlarged collaterals [16]. Variceal haemorrhage at presentation however, does not influence overall survival [17].
Figure 1: Sonogram shows replacement of main portal vein with
multiple serpiginous, anechoic channels (arrow) that on color Doppler
interrogation revealed slow flow.
Ultrasonography is the initial investigation that reveals numerous anechoic vascular channels at porta. Gold standard for diagnosis of CTPV is conventional angiography. However, MR angiography is as accurate as conventional angiography. A prophylactic surgery in this case is debatable with some surgeons intervening only on development variceal hemorrhage. Endoscopic management in the form of band ligation or sclerotherapy are preferred procedures. Portosystemic shunt is created in those who fail to benefit from endoscopic measures. [17] PV thrombosis with CTPV limits the success of TIPS since accessibility of PV via transjugular route becomes difficult in chronically thrombosed vein [18]. Moreover, passage of wire through one of the collaterals across the occluded segment is either difficult or impossible. Hence, PV thrombosis with CTPV, a contraindication to TIPS [18]. Jourabchi however, described a case of CP associated CTPV where TIPS was performed employing a combined transjugular and transhepatic approach [18].
Portal Biliopathy
Collaterals in CTPV can mechanically obstruct the biliary track giving rise to Portal Biliopathy (PB) (Figure 2)[19]. Occurrence of PB in CP is a rare phenomenon [19, 20]. These vessels may cause ischemia induced fibrosis of the track. Majority do not manifest any symptoms of biliary obstruction [16]; chronic cholestasis, biliary pain and calculus may occur in a few. However, symptoms related to portal hypertension are more frequent than symptoms of chronic cholestasis [21]. Rana et al. described endoscopic ultrasonography (EUS) features of PB in a female suffering from acute severe pancreatitis [20]. EUS features include prominent common bile duct with anechoic serpentine veno-venous collaterals around the biliary tree. ERCP however, is the key investigation; although MRCP is equally accurate for diagnosing PB[21]. MRCP with MR portography has the additional advantage of distinguishing bile duct varices from biliary duct calculi. Cholangiographic findings include segmental upstream dilation, caliber irregularity, stricture, extrinsic impression due to collaterals (-the pseudocholangiocarcinoma sign) [21]. The strictures are typically smooth unlike those of sclerosing cholangitis [21]. Intervention is required in patients with a dominant biliary stricture and features of obstructive jaundice. In patients with a shuntable vein, a portosystemic shunt is performed or else endotherapy is preferred [21].
Figure 2: CECT coronal reformation demonstrates dilated common bile
duct (green arrows) surrounded by numerous collaterals in a setting of
portal biliopathy.
Gallbladder Wall Varices
Another set of collaterals in PV thrombosis includes gallbladder wall varices (GWV) (Figure 3) which are seen in 30 % of patients with PV thrombosis (Chawla et al.). These are portosystemic shunts between cystic vein branch of the PV either to systemic anterior abdominal wall veins or to the patent PV branches within the liver [14]. On sonography, the GWV appear as anechoic serpentine channels that show a continuous low velocity signal typical of portal venous system [14]. Their presence does not correlate with the site and extent of PV thrombosis [14]. The varices may reduce the distensibility of gall bladder [21] or can give rise to hemobilia or intraabdominal hemorrhage. There is, however, no alteration in emptying of gall bladder or lithogenicity of bile [21]. Clinical implication of GWV include variceal bleed (seen in 1%) [22] and caution during biliary track surgeries for risk of hemorrhage.
Figure 3: Sonogram depicts dilated venous channels in the wall of gall
bladder.
Transient Hepatic Attenuation Difference
Transient hepatic attenuation difference (THAD) occurs due to regional diminution in PV flow [23]; the diminution can be absolute or relative. This leads to non-dilution of iodinated hepatic artery blood in that particular region and forms the basis of increased attenuation (difference in attenuation) in these areas [24]. The compensatory increase in hepatic artery flow that occurs in PV thrombosis accentuates this phenomenon [24]. Morphologically THAD has been classified into Lobar multisegmental, Sectorial, Polymorphous and Diffuse [23].
THAD is seen on arterial phase of CT as an area of increased attenuation that returns to normal or near normal on portal venous phase [25]. Similar findings on MRI have been called Transient Hepatic Intensity Difference (THID) [26]. THAD by itself is not pathological but indicates an associated pathology.
Pancreatitis-associated THAD may arise because of inflammation induced increase in arterial inflow (polymorphous type) [27] or thrombosis in portal, splenic or superior mesenteric veins (sectorial or diffuse type). A sectorial type occurs in the setting of thrombosis of portal vein and typically has a wedge shaped or atleast one straight border [23, 27]. When the thrombus is present in the main PV trunk, collaterals in the peri-hilar region maintain perfusion of the central portion. The periphery however, continues to receive undiluted contrast carried by hepatic artery branches with consequent high attenuation of the periphery. Such a pattern is called central-peripheral subtype of diffuse THAD (Figure 4) [27].
Figure 4a: CECT arterial phase demonstrates a sectorial type of transient
hepatic attenuation difference with a straight border (solid arrow).
Also note thrombosis in a tributary of portal vein (arrow) with fluid
collection in the body of pancreas.
Figure 4b: CECT venous phase shows near complete resolution of
transient hepatic attenuation difference with thrombosis in a tributary
of portal vein (arrow).
THAD that occurs due to thrombosis of SV, SMV or partial thrombosis or compression of PV involves an entire lobe [24]. Such an observation is based on the fact that portal blood flow is streamlined with superior mesenteric venous blood contributing posterolateral column of blood in the PV and splenic venous blood occupying an anteromedial place [28]. Hence, obstruction of splenic vein or anteromedial portion of PV produces left lobar THAD, while pathology of SMV or posterolateral PV exhibits right lobar THAD [24]. Since this ultimately affects portal venous inflow, typically there is presence of one straight border.
Splenic Complications Due to Splenic Vein Thrombosis
Pancreatitis associated splenic complications manifest as infarction, spontaneous rupture of spleen (SSR) or subcapsular hematoma [29]. Involvement of the organ may occur via enzymatic dissection between splenic peritoneum and capsule or dissection though the splenic capsule or both [29]. Since pancreatic tail lies in anatomic contiguity with splenic hilum, inflammation around the pancreatic tail is a prerequisite for development of such complications. These complications are more pronounced with pancreatitis associated SV thrombosis (Malka et al.) [29].
SSR is an uncommon surgical emergency. Clinical features include left hypochondriac pain, hypotension, guarding and rigidity [30, 31]. Kehr’s sign may be positive [30]. High index of suspicion is necessary and any patient of acute pancreatitis presenting with signs of shock should be evaluated for SSR. Management depends on hemodynamic stability, degree of hemoperitoneum and severity of splenic injury [31]. No active intervention is required if the patient is hemodynamically stable; these patients can be kept under close clinical and sonographic monitoring. Conservative approach was employed by Mujtaba et al. in a hemodynamically stable patient of acute pancreatitis (with crohn’s disease) who developed SSR following SV thrombosis [31]. Similarly, Rypens et al. [30]suggested a wait and watch policy since pancreatitis associated splenic complications may potentially regress over time. On the contrary, surgical intervention is warranted if the patient has precipitous drop in blood pressure or develops signs of peritonitis [31].
Bowel Wall Infarction
A thrombosis in mesenteric venous system can also be a harbinger of an acute complication. Thrombotic occlusion of veins may result in bowel wall infarction [32, 33, 34]. Extent and severity of infarction along with other co-morbid conditions predict the final outcome. Ischemic insult, if mild, heals with stenosis of lumen [32] and may mimic a neoplastic process [33]. On the other hand, gangrene [34] or perforation [34, 35, 36] of the bowel ensues if the inciting ischemic injury is severe. The gut mucosa may reveal ulceration and there may be associated mesenteric panniculitis [32]. Bowel infarctions secondary to pancreatitis associated thrombotic venous states have been described for jejunum [32, 36, 37] and colon [34, 35]. Nottle et al. [35] reported a case of pancreatitis associated colonic infarction with perforation treated by subtotal colectomy and diversion ileostomy followed at a later date by ileosigmoid anastomosis.
Portal Vein-Pseudocyst Fistulisation
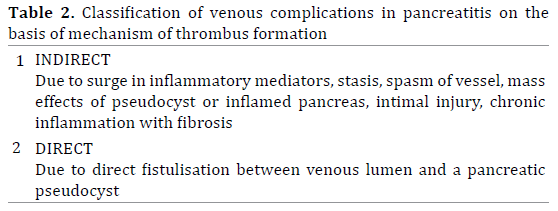
Venous thrombosis in pancreatitis can also be classified on the basis of mechanism of thrombosis (table 2): indirect, wherein procoagulant inflammatory mediators increase or direct wherein pancreatic pseudocyst empties itself directly into venous lumen (vein-pseudocyt fistulisation). The latter has been described usually in the context of PV. Portal veinpseudocyst fistula may present clinically as vague abdominal pain [38] or widespread fat necrosis [38, 39, 40] with increased morbidity. Hammar et al. described a patient with residivating oligoarthritis, subcutaneous, bursal and osseal necrosis in the setting of Pancreatic pseudocyst-portal vein fistula [41].
Pseudocyst-portal vein fistula is commonly seen in males particularly with a history of alcohol-induced pancreatitis [38]. The mechanism of fistulisation involves erosion of the venous wall by the uninhibited enzymes from an adjacent pseudocyst with initial thrombus formation. Later, there is lysis of the thrombus and filling in of the vein with pancreatic succus [42]. Since the pseudocyst is a high pressure zone, devastating bleeding is rare [38].
MRI may delineate the fistula as a T2 hyperintense tract joining the pseudocyst and the vein [38]. ERCP may help if the pancreatic duct communicates with the pseudocyst [15]. The role of ERCP may be limited if the pancreatic duct has strictures or calcifications clogging the duct [38]. Percutaneous transhepatic portography may also be helpful [38]. In a few cases, however, diagnosis was established on autopsy [38, 43, 44]. Differentials for a low attenuation of portal vein include a portal vein-pseudocyst fistula, a bland thrombosis in hypercoagulable states or mass effect by tumor or lymph nodes. The portal vein-pseudocyst fistula may reveal complex fluid in the PV on ultrasonography. The other two conditions are similar except the extrinsic mass will be seen causing narrowing of the PV [38].
Patients with mild symptoms can be managed conservatively while reserving aggressive surgical intervention for symptomatic ones. Definitive surgical methods include PV plasty [38]; diversion of pancreatic secretions may be attempted at a later date when acute symptoms subside [38].
Miscellaneous
1) Infarction of liver is uncommon owing to dual blood supply by PV and hepatic artery with PV constituting 80% of the share. Pancreatitis associated hepatic infarction is a rare entity [45, 46]; postulated to be caused by marked diminution of blood supply to liver due to PV thrombosis [45, 46, 47]. Walsh et al. [48] described a case of pancreatitis associated hepatic infarction where severe reduction in hepatic inflow occurred due to both PV thrombosis as well as shunting of blood across iatrogenically created portosystemic shunt.
2) While thrombosis of veins in peripancreatic region is a common event, thrombosis in extrasplanchnic system is sparingly reported. Parikh et al. described thrombosis of superior and inferior vena cava, axillary, subclavian and common iliac veins without involvement of splanchnic veins [49]. Similarly many authors have also described thrombosis of inferior vena cava [50, 51], pulmonary artery [52], inferior vena cava and renal veins [53], inferior vena cava with pulmonary artery [54]. Of particular interest is Phlegmasia cerulea dolens, a form of deep venous thrombosis with a proximal localization of the blockage, described by Molacek et al. in the setting of acute hemorrhagicnecrotising pancreatitis [55]. The condition most frequently involves ileofemoral region and is usually seen in terminal stages of malignancies [55].
HEMORRHAGIC COMPLICATIONS IN PANCREATITIS
Pancreatitis associated hemorrhagic complications may be both arterial as well as venous. Rarely, the venous erosion by tryptic enzymes may not be contained (unlike pseudocyst- portal vein fistula). Instead, erosion of venous wall may result into a massive abdominal haemorrhage[56]. Instances have been described for portal [56, 57] as well as SV [58]. On ultrasonography, fluid with echoes can be demonstrated. However, CT is the modality of choice and needle aspiration of serosanguinous fluid is diagnostic. Management involves placement of a stent graft across the mural defect [56, 57].
IMPAIRED VENOUS DRAINAGE IN PANCREATITIS
Pancreatitis associated partial thrombosis or extrinsic compression by a pseudocyst may lead to impaired venous drainage. Such a non-thrombotic, compressive effect of pseudocyst [59, 60] has been described for left renal and testicular veins. The diminution in drainage gave rise to engorgement of venous bed of testis (secondary varicocele). Such an occurrence is extremely rare and has been reported only twice [59, 60]. The patients present with heaviness and vague pain in scrotum. Ultrasonography shows dilated, tortuous venous channels located posterolateral to the testis. A CECT demonstrates compression of the draining veins. Management in both cases included drainage of pseudocyst fluid into stomach with resolution of symptoms [59, 60].
To conclude, venous manifestations in pancreatitis are numerous; majority arising due to chronic venous thrombosis and consequent collateralization. There can be pressure effects on the veins hampering venous return or there can be massive hemorrhage following enzymatic digestion of the venous wall. This article attempts to describe venous complications associated with pancreatitis.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Mallick IH, Winslet MC. Vascular complications of pancreatitis. JOP 2004; 5 (5): 328-37. [PMID: 15365199]
- Park WS, Kim HI, Jeon BJ, Kim SH, Lee SO. Should anticoagulants be administered for portal vein thrombosis associated with acute pancreatitis? World J Gastroenterol 2012; 18(42): 6168-71. [PMID: 23155349]
- Sakorafas GH, Tsiotou AG. Splenic-vein thrombosis complicating chronic pancreatitis. Scand J Gastroenterol 1999; 34: 1171-7. [PMID: 10636062]
- Izbicki JR, Yekebas EF, Strate T, Eisenberger CF, Hosch SB, Steffani K, Knoefel WT. Extrahepatic portal hypertension in chronic pancreatitis: an old problem revisited. Ann Surg 2002; 236(1): 82-9. [PMID: 12131089]
- Wang L, Liu GJ, Chen YX, Dong HP, Wang LX. Sinistral portal hypertension: clinical features and surgical treatment of chronic splenic vein occlusion. Med PrincPract 2012; 21(1):20-3. [PMID: 22024761]
- Kokabi N, Lee E, Echevarria C, Loh C, Kee S. Sinistral portal hypertension: presentation, radiological findings, and treatment options - a case report. J Radiol Case Rep 2010; 4(10):14-20. [PMID: 22470692]
- Rösch W, Lux G, Riemann JF, Hoh L. [Chronic pancreatitis and the neighboring organ. Fortschr Med 1981; 99(29): 1118-21. [PMID: 7262798]
- Patrono D, Benvenga R, Moro F, Rossato D, Romagnoli R, Salizzoni M. Left-sided portal hypertension: Successful management by laparoscopic splenectomy following splenic artery embolization. Int J Surg Case Rep 2014; 5(10): 652-5. [PMID: 25194596]
- Köklü S, Coban S, Yüksel O, Arhan M: Left-sided portal hypertension. Dig Dis Sci 2007; 52: 1141–1149.
- Agarwal AK, Raj Kumar K, Agarwal S, Singh S. Significance of splenic vein thrombosis in chronic pancreatitis. Am J Surg 2008; 196(2): 149-54. [PMID: 18585674]
- Burbige EJ, Tarder G, Carson S, Eugene J, Frey CF. Colonic varices. A complication of pancreatitis with splenic vein thrombosis. Am J Dig Dis 1978; 23(8): 752-5. [PMID: 685944]
- Liu Q, Song Y, Xu X, Jin Z, Duan W, Zhou N. Management of bleeding gastric varices in patients with sinistral portal hypertension. Dig Dis Sci 2014; 59(7): 1625-9. [PMID: 24500452]
- Heider TR, Azeem S, Galanko JA, Behrns KE. The natural history of pancreatitis-induced splenic vein thrombosis. Ann Surg 2004; 239 (6): 876-80. [PMID: 15166967]
- Chawla Y, Dilawari JB, Katariya S. Gallbladder varices in portal vein thrombosis. AJR Am J Roentgenol 1994; 162(3): 643-5. [PMID: 8109513]
- Brown A, Malden E, Kugelmas M, Kortz E. Diagnosis of pancreatic duct-portal vein fistula; a case report and review of the literature. J Radiol Case Rep 2014; 8(3): 31-8. [PMID: 24967026]
- Mensier A, Bounoua F, Beretvas G, Mosoi A, Dardenne S. Kissing gastric ulcers causing acute pancreatitis and portal biliopathy: what's the link? JOP 2013; 14(6): 646-8. [PMID: 24216552]
- Janssen HL, Wijnhoud A, Haagsma EB, van Uum SH, van Nieuwkerk CM, Adang RP, Chamuleau RA, van Hattum J, Extrahepatic portal vein thrombosis: aetiology and determinants of survival. Gut 2001; 49 (5): 720-4. [PMID: 11600478]
- Jourabchi N, McWilliams JP, Lee EW, Sauk S, Kee ST. TIPS Placement via Combined Transjugular and Transhepatic Approach for Cavernous Portal Vein Occlusion: Targeted Approach. Case Rep Radiol 2013; 2013: 635391. [PMID: 23401834]
- Stefanescu H, Grigorescu M, Tantau M, Badea R, Cormos R. Portal biliopathy--a lesser known complication of portal hypertension. Case report and review of the literature. Rom J Gastroenterol. 2003; 12(4): 309-13. [PMID: 14726977]
- Rana SS, Bhasin DK, Rao C, Singh K. Portal hypertensive biliopathy developing after acute severe pancreatitis. Endosc Ultrasound. 2013; 2(4): 228-9. [PMID: 24949402]
- Dhiman RK, Behera A, Chawla YK, Dilawari JB, Suri S. Portal hypertensive biliopathy. Gut. 2007; 56(7): 1001-8. [PMID: 17170017]
- Ralls PW, Mayekawa DS, Lee KP, Colletti PM, Johnson MB, Halls JM. Gallbladder wall varices: diagnosis with color flow Doppler sonography. J Clin Ultrasound. 1988; 16(8): 595-8. [PMID: 3152408]
- Ravikumar H, Singh J, Kalyanpur A. Transient Hepatic Attenuation Difference (Thad) - A Case Report. Ind J RadiolImag 2006; 4: 441-444.
- Wong H, Desser TS, Jeffrey RB. Transient Hepatic Attenuation Differences in Computed Tomography from Extrahepatic Portal Vein Compression. Radiology Case Reports 2008; 3:113.
- Chen WP, Chen JH, Hwang JI, Tsai JW, Chen JS, Hung SW, Su YG, Lee SK. Spectrum of transient hepatic attenuation differences in biphasic helical CT. AJR Am J Roentgenol. 1999; 172(2): 419-24. [PMID: 9930795]
- Colagrande S, Centi N, Galdiero R, Ragozzino A. Transient hepatic intensity differences: part 1, Those associated with focal lesions. AJR Am J Roentgenol 2007; 188(1): 154-9. [PMID: 17179358]
- Colagrande S, Centi N, La Villa G, Villari N. Transient hepatic attenuation differences. AJR Am J Roentgenol. 2004; 183(2): 459-64. [PMID: 15269041]
- Gallix BP, Reinhold C, Dauzat M, Bret PM. Streamlined flow in the portal vein: demonstration with MR angiography. J MagnReson Imaging 2002; 15(5): 603-9. [PMID: 11997903]
- Patil PV, Khalil A, Thaha MA. Splenic parenchymal complications in pancreatitis. JOP. 2011; 12(3): 287-91. [PMID: 21546711]
- Purushothaman K, Borowski DW. Unusual presentation of spontaneous splenic haematoma due to severe pancreatitis: a cautionary tale. BMJ Case Rep 2012. [PMID: 23148400]
- Mujtaba G, Josmi J, Arya M, Anand S. Spontaneous splenic rupture: a rare complication of acute pancreatitis in a patient with Crohn's disease. Case Rep Gastroenterol. 2011; 5(1): 179-82. [PMID: 21552441]
- Kim YI, Choe KJ, Choi KW. Ischemic jejunal stenosis following acute pancreatitis with mesenteric panniculitis. Korean J Gastroenterol 1991; 23: 930-935.
- Cho YD, Hong SJ, Moon JH, et al. Stenosis of the colon due to chronic pancreatitis mimicking colon cancer. Korean J GastrointestEndosc 1998; 18: 605-610.
- Katz P, Dorman MJ, Aufses AH Jr. Colonic necrosis complicating postoperative pancreatitis. Ann Surg 1974; 179(4): 403-5. [PMID: 4815897]
- Nottle P. Colonic infarction and pancreatitis: a case report. Aust N Z J Surg 1980; 50(2): 184-5. [PMID: 6930238]
- Chai JY, Yun SI, Bae SS, Chae HB, Park SM, Youn SJ, Park JW, Bae IH, Kim SH, Song HG, Wang JH. [A case of jejunal infarction and perforation due to acute pancreatitis. Korean J Gastroenterol 2004; 43: 120-4. [PMID: 14978369]
- Griffiths RW, Brown PW Jr. Jejunal infarction as a complication of pancreatitis. Gastroenterology. 1970; 58(5): 709-12. [PMID: 5444175]
- Raza SS, Hakeem A, Sheridan M, Ahmad N. Spontaneous pancreatic pseudocyst-portal vein fistula: a rare and potentially life-threatening complication of pancreatitis. Ann R CollSurgEngl 2013; 95: e7-9. [PMID: 23317711]
- Delcenserie R, Bental A, Goll A, Butel J, Du98pas JL. [Pancreatic-portal fistula and subcutaneous fat necrosis. GastroenterolClin Biol. 1994; 18(12): 1132-7. [PMID: 7750687]
- Rabache A, Crinquette JF, Vermersch A, Cuingnet P, Maunoury V, Hanon D, Lescut J. [Pancreatic-portal fistula. A rare complication of chronic pancreatitis GastroenterolClinBiol 1994; 18(12): 1138-41. [PMID: 7750688]
- Hammar AM, Sand J, Lumio J, Hirn M, Honkonen S, Tuominen L, Nordback I. Pancreatic pseudocystportal vein fistula manifests as residivatingoligoarthritis, subcutaneous, bursal and osseal necrosis: a case report and review of literature. Hepatogastroenterology 2002; 49(43): 273-8. [PMID: 11941974]
- Dawson BC, Kasa D, Mazer MA. Pancreatic pseudocyst rupture into the portal vein. South Med J 2009; 102(7): 728-32. [PMID: 19561436]
- Skarsgard ED, Ellison E, Quenville N. Spontaneous rupture of a pancreatic pseudocyst into the portal vein. Can J Surg 1995; 38(5): 459- 63. [PMID: 7553473]
- Packeisen J, Klingen D, Grezella F. Spontaneous rupture of a pancreatic pseudocyst into the portal vein. Z Gastroenterol 2001; 39(11): 961-4. [PMID: 11778155]
- Kim HS, Hong SH, Park HS, Lee ES, Kang IW. Hepatic Infarction Complicating Acute Pancreatitis: A Case Report. J Korean RadiolSoc 2000; 43(1): 73-76.
- Kim BC, Joo KR, Lee HS, Jeong YK, Suh HS, Kim DH, Park NH, Park JH. A Case of Chronic Pancreatitis Associated with Liver Infarction and AcrodermatitisEnteropathica. Korean J Intern Med 2002; 17(4): 263-5. [PMID: 12647643]
- Maruyama M, Yamada A, Kuraishi Y, Shibata S, Fukuzawa S, Yamada S, Arakura N, Tanaka E, Kadoya M, Kawa S. Hepatic Infarction Complicated with Acute Pancreatitis Precisely Diagnosed with GadoxetateDisodiumenhanced Magnetic Resonance Imaging. Intern Med 2014; 53(19): 2215- 21. [PMID: 25274233]
- Walsh TJ, Eggleston JC, Cameron JL. Portal hypertension, hepatic infarction, and liver failure complicating pancreatic islet autotransplantation. Surgery 1982; 91(4): 485-7. [PMID: 6801798]
- Parikh H, Shukla A, Aswani Y, Bhatia S. Multiple extrasplanchnic venous thromboses: a rare complication of pancreatitis. A case report. JOP 2012; 13(3): 317-9. [PMID: 22572142]
- Stringer MD, Michell M, McIrvine AJ. Inferior vena caval thrombosis complicating acute pancreatitis. Case report. ActaChirScand 1988; 154(2): 161-3. [PMID: 3354298]
- Peillon C, Manouvrier JL, Testart J. Inferior vena cava thrombosis secondary to chronic pancreatitis with pseudocyst. Am J Gastroenterol 1991; 86(12): 1854-6. [PMID: 1962640]
- Zhang Q, Zhang QX, Tan XP, Wang WZ, He CH, Xu L, Huang XX. Pulmonary embolism with acute pancreatitis: a case report and literature review. World J Gastroenterol 2012 14; 18(6): 583-6. [PMID: 22363127]
- Mukund A, Gamanagatti S, Saraya A. Chronic pancreatitis causing thrombotic occlusion of IVC and renal veins. Trop Gastroenterol 2013; 34(1): 39-41. [PMID: 23923375]
- Ohta H, Hachiya T. A case of inferior vena cava thrombosis and pulmonary embolism secondary to acute exacerbation of chronic pancreatitis: a rare finding in radionuclide venography. Ann Nucl Med 2002; 16(2): 147-9. [PMID: 12043910]
- Molacek J, Treska V, Baxa J, Duras P, Vesely V. Phlegmasiaceruleadolens as a complication of a severe form of acute hemorrhagicnecrotizing pancreatitis. Blood Coagul Fibrinolysis. 2008; 19(1):98-100. [PMID: 18180625]
- Charvat F, Maskova J, Belina F, Buric I, Lacman J, Fuksa Z, Vrana J. Portal vein erosion: a rare hemorrhagic complication of acute pancreatitis treated by percutaneous stent-graft placement. J VascIntervRadiol. 2010; 21(3):411-2. [PMID: 20171562]
- Lacman J, Buric I, Charvát F, Masková J, Fuksa Z, Pudil J, Belina F. [Multidisciplinary cooperation in the management of serious bleedings complicating necrotizing pancreatitis--a case review. RozhlChir. 2008; 87(10): 507-11. [PMID: 19110942]
- Müller CH, Lahnert U, Schafmayer A, Lankisch PG. Massive intraperitoneal bleeding from tryptic erosions of the splenic vein. Another cause of sudden deterioration during recovery from acute pancreatitis. IntJPancreatol. 1999; 26(1): 49-52. [PMID: 10566158]
- Dixon JM, Armstrong CP, EreminO.Varicocele caused by a pancreatic pseudocyst.Gut 1983; 24(5): 438-40. [PMID:6840618]
- Aswani Y, Hira P. Secondary Varicocele Caused by Pancreatic Pseudocyst Obstructing Testicular Venous Drainage. JOP. J Pancreas (Online) 2013; 14(6): 674-675. [PMID: 24216560]






