Introduction: Rehabilitation of patients with chronic obstructive pulmonary disease (COPD) is recommended on basis of solid evidence. However, implementation of guidelines for COPD rehabilitation has shown to be difficult and many patients are not referred to primary care rehabilitation.
Aim: This study aims to examine if existing webbased information is sufficient to support referral of patients to COPD rehabilitation programs and if available information reflects the deliverance of recommended COPD rehabilitation.
Methods: The region of Southern Denmark (RSD) was chosen as case for this study. We scrutinized all information on the website www.sundhed.dk related to services for COPD patients. We registered information on following items: 1) Referral procedure, 2) Target groups, 3) Content of programs, 4) Setting, 5) Timetable, 6) Logistics and 7) Waiting time. Subsequently, we contacted all municipalities to complement this information.
Results: According to information on the website, all 22 municipalities in RSD offered at least one COPD rehabilitation program. Complete information on referral procedure and target group was present in 15 and 4 cases respectively. Seventeen municipalities had no information on waiting time and/or timetable. Direct contact to municipalities supplemented the information but still important data were unavailable.
Conclusion: The study demonstrated variable and insufficient web-site information for COPD rehabilitation in municipalities. More focus on readily accessible information might support referrals and thereby implementation on rehabilitation guidelines.
Keywords
Pulmonary disease; Rehabilitation; Primary care; Patient education; Chronic obstructive lung disease.
Introduction
The effects of rehabilitation of patients with chronic obstructive lung disease (COPD) are well proven and therefore widely recommended.[1-3]
Referral of patients to rehabilitation programs relies on readily accessible and adequate information for both patients and referring professionals about the content and availability of the programs. In Denmark, information on rehabilitation services is presupposed to be available on the national website. Such readily accessible information is important, since COPD rehabilitation increasingly is carried out by municipalities in Denmark and thus often implies handovers between health care settings.[4] Furthermore, existing rehabilitation programs should comprise the recommended content of rehabilitation services.[5] and finally, the overall capacity should match the actual demand for COPD rehabilitation. Inadequate information on these issues could potentially act as barriers and influence patient and referrer adherence to rehabilitation services.
This study aims to examine the usability of web-based information to support referral – mainly from general practitioners (GP’s) – of patients to COPD rehabilitation programs in Danish municipalities and to assess whether the information reflects the deliverance of recommended COPD rehabilitation.
Material and Methods
Information about available COPD rehabilitation services was from the outset obtained from sunhed.[4] A preliminary pilot search on the website showed that variation in services within regions was greater than variation between regions. Therefore, we selected a single region as case for this study. We chose the Region of Southern Denmark (RSD) due to its average size and central location. RSD is one of five Danish regions and has a mixture of urban and rural population of 1.2 million people.
We scrutinized all information on the website related to services for COPD patients. In relation to uploaded information on COPD rehabilitation programs we registered the presence or absence of data concerning following items: 1) Referral procedure, 2) Target groups, 3) Content of each program (elements of rehabilitation ), 4) Type of program (individualized and/or class), 5) Location, 6) Day of week/time of day, and 7) Waiting time.
Subsequently, we e-mailed and telephoned all 22 municipalities to complement information about current rehabilitation programs. We collected all data during the first quarter of 2016.
Results
Data from www.sundhed.dk
We used the definition from the Danish national clinical guideline that broadly defines rehabilitation as a service that as least must contain physical training and that can be combined with one or more of the following activities; patient education, dietary advice, smoking cessation course, psychosocial support.[5] According to this definition, all 22 municipalities in RSD offer at least one rehabilitation program for patients with COPD and 12 out of 22 municipalities offer more than one program.
For Figure 1, we retrieved information from the national website. The left part of the figure shows present information on referral procedures and patient eligibility to rehabilitation programs. The right part displays additional information found on the website relevant for referrers and patients prior to deciding about the appropriateness of referring and participating in rehabilitation (e.g. content of programs, location/time of day and waiting time for starting rehabilitation). Information on the target group (mild/moderate/severe COPD) was specified in four of the 22 municipalities. Participation in the majority of programs required referrals from a health care professional, for few programs it was possible to sign up by direct patient contact. The national website contained information on referral procedures (including location number and which phrases to use for referral) for 15 municipalities while six only had information on referral procedures for part of their COPD programs. Fifteen municipalities stated the location of rehabilitation for all of their programs, three had only information on location for some programs and four had no information of location at all. Two municipalities gave information of day and time point of all rehabilitation programs and three only for some programs. Two municipalities informed about waiting times on www.sundhed.dk for all their COPD programs while three only exposed information on waiting times for some of their programs. In total seventeen municipalities had no information on waiting time on the national website at all.
Figure 2 displays the elements of the rehabilitation programs in the municipalities. These elements are in some municipalities a part of a generic program, in other separate courses. All 22 communities provided a physical element for the COPD patient group. Provision of some of the other elements shows minor variation.
Data obtained by mail/phone
For most municipalities, we were not able to find comprehensive information on the national website. For a number of the previous mentioned seven items information was not available. Therefore, we tried to collect additional information by contacting municipalities by phone/mail. Despite this further effort, still some information was not attainable due to either insufficient registration or lack of access to diagnosis specific data.
Most municipalities stated that they predominantly performed class-based rehabilitation. Within classes, individual adjustment of the program was possible in most programs. Eight municipalities had continuously uptake of patients for class-based rehabilitation, a routine that profoundly affected waiting times positively. Thus, seven out of eight communities with continuously uptake had waiting times between 0 and 2 weeks, while the mean waiting time for the rest of the communities was 8 weeks. These figures cover large differences though (Figure 3).
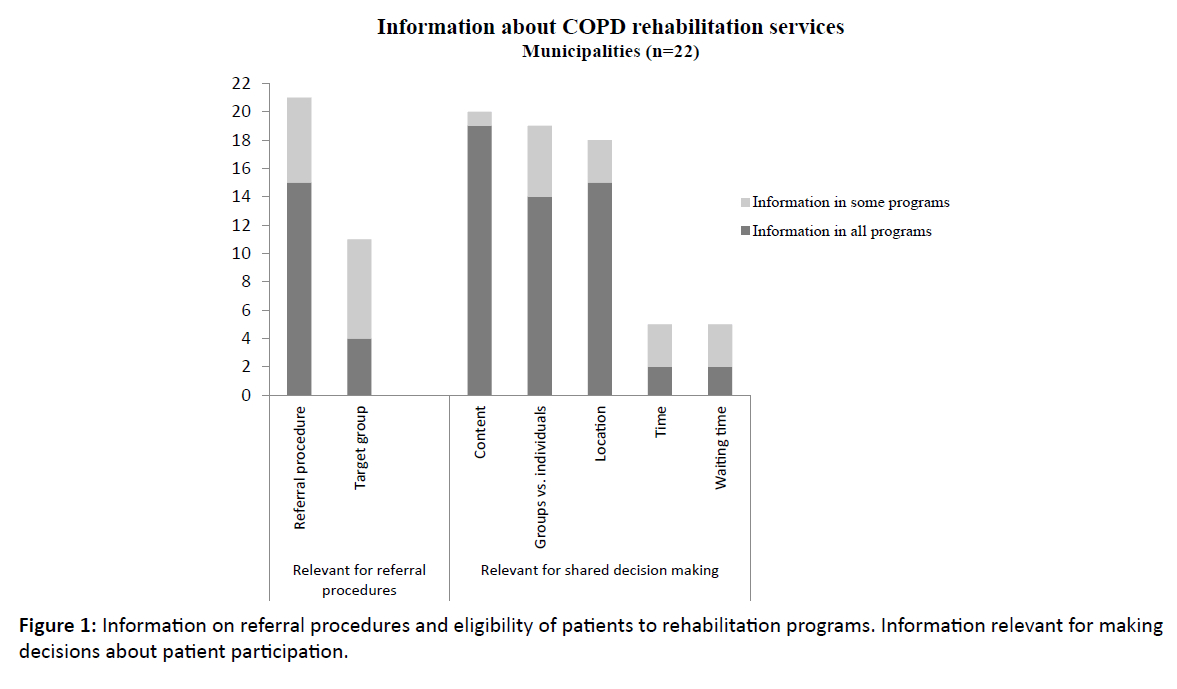
Figure 1: Information on referral procedures and eligibility of patients to rehabilitation programs. Information relevant for making decisions about patient participation.
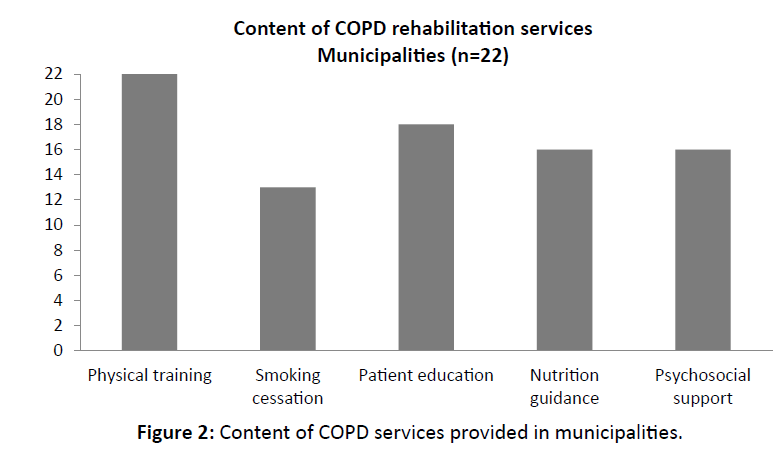
Figure 2:Content of COPD services provided in municipalities.
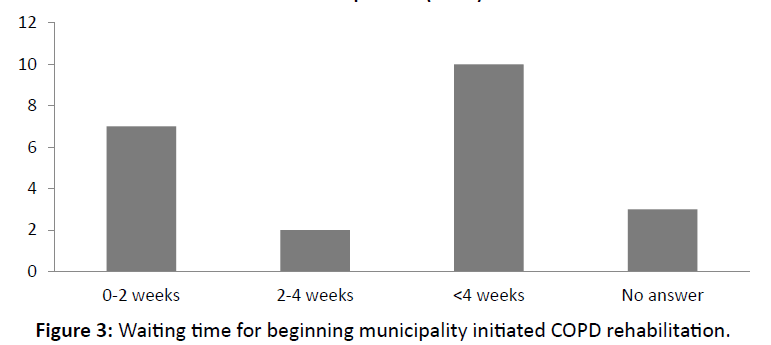
Figure 3:Waiting time for beginning municipality initiated COPD rehabilitation.
In terms of yearly activity, some municipalities had data on numbers of referrals; others had data on the number of patients commencing a program, while four municipalities had no information on either. From available data, we the average uptake in the municipalities to approximately 70 patients per year. If this number is representative for all municipalities, this corresponds to a yearly uptake of about 1500 COPD patients in the region. Twelve of the contact-persons stated that they could increase their capacity on demand.
Discussion
Internationally, there is a growing body of evidence on the positive effects of COPD rehabilitation on morbidity, mortality and quality of life.[2,3,6] However, recommendations regarding rehabilitation for this patient group are often not implemented in practice.[7,8] Awareness of this paradox has led to a range of efforts to identify barriers and facilitators in order to increase the number of patients participating and completing rehabilitation programs.[9-16] Detected barriers include uncertainties about referral procedures, lack of knowledge about availability and composition of programs, transport logistics and shortage of capacity.[10,17,18]
In Denmark, the website [4] is the national platform designed to provide information in order to support decision making regarding referral and patient participation in different health care services. We therefore investigated whether the information on this platform was suited and sufficient to support referral of patients to COPD rehabilitation programs. Furthermore, we used this information to assess if current services in 22 communities in a Danish region meet the recommendations for delivering COPD rehabilitation as suggested in a newly published Danish national rehabilitation guideline.[5] In order to succeed in meeting the COPD rehabilitation guideline, information about existing rehabilitation programs should be easily accessible for GP’s and others who refer patients and sufficient information should be available for patients to determine if the program is appropriate.
We found a substantial variation between providers in the amount and type of information given on the website and demonstrated that relevant information for COPD rehabilitation is insufficient in many cases. Together with an apparent diversity in the content of the programs, both in respect to number and nature of services, this variation will most likely lead to inconsistency in the provision of COPD rehabilitation across the region.
In case of inadequate information about available programs, the referring GP’s potentially will have to contact the provider to obtain additional information used to make informed decision on referring a patient to rehabilitation. Difficulties to access to such information are highlighted in a recent Danish study looking at challenges in exchange of information between municipalities and general practice. Nearly one third of GPs stated insufficient knowledge about municipal services as the reason for not referring patients.[19] An Australian study looking at barriers and facilitators for referral of COPD patients to rehabilitation describes similar experiences.[20]
Early rehabilitation after hospital discharge for exacerbation has shown to reduce readmission rates for COPD patients.[3] This is one reason why early rehabilitation is an important challenge to address for providers of COPD rehabilitation. The Danish national guideline defines early rehabilitation as a program starting less than four weeks after discharge, but the majority of municipalities report waiting times well above this time limit. Furthermore, as rehabilitation usually is carried out in class-based settings initiated with more than monthly intervals, the prerequisites for meeting the guideline for newly discharged patients seems often not to be present.
The novel rehabilitation recommendations include new groups for rehabilitation, therefore sufficient capacity of services is essential to comprise the enlarged group of COPD patients suitable for rehabilitation. In the Region of Southern Denmark, the hospitals discharge approximately 3000 patients with COPD every year. Added to complementary well-accepted target groups, the demand for rehabilitation clearly exceeds the current capacity of the municipalities. However, more than half of the municipalities stated that they would be able to increase capacity, so the main challenge seems to be related to facilitation of the referral procedure by improvement of information and cooperation between health care settings.
Conclusion
This study found varying and partly inadequate information for the provision of primary care COPD rehabilitation in a Danish region. This variation could potentially lead to inconsistency in the implementation of COPD rehabilitation guidelines. There are still a number of challenges for most municipalities in the Region of Southern Denmark in order to make eligible COPD patients participate in rehabilitation programs and especially to provide timely rehabilitation for newly discharged patients. More attention is needed in the deliverance of updated web-based information to support referrals of patients and to align present services to match actual recommendations regarding COPD rehabilitation.
Ethical Approval
The study do not include patient related data, therefore it did not need any approval from the Danish Regional Ethics Committee.
Source of Funding
No funding was received for the study. The study was funded internal at the Centre for Quality.
References
- Johnston K, Grimmer-Somers KPulmonary rehabilitation: Overwhelming evidence but lost in translation? Physiotherapy Canada Physiotherapie Canada 2010; 62: 368-373
- McCarthy B, Casey D, Devane D, Murphy K, Murphy E, et alPulmonary rehabilitation for chronic obstructive pulmonary diseaseCochrane Database Syst Rev 2015; 2: Cd003793
- Puhan MA, Gimeno-Santos E, Scharplatz M, Troosters T, Walters EH, et alPulmonary rehabilitation following exacerbations of chronic obstructive pulmonary diseaseCochrane Database Syst Rev 2011; 10: Cd005305
- https://www.sundhed.dk/
- Board DNHNational clinical guideline for the Rehabilitation of patients with chronic Obstructive Pulmonary DiseaseBoard TDNH 2014
- Garcia-Aymerich J, Farrero E, Felez MA, Izquierdo J, Marrades RM, et alRisk factors of readmission to hospital for a COPD exacerbation: A prospective studyThorax 2003; 58: 100-105
- Johnston K, Grimmer-Somers K, Young M, Antic R, Frith PWhich chronic obstructive pulmonary disease care recommendations have low implementation and why? A pilot studyBMC Res Note 2012; 5: 652
- Johnston KN, Young M, Grimmer-Somers KA, Antic R, Frith PAWhy are some evidence-based care recommendations in chronic obstructive pulmonary disease better implemented than others? Perspectives of medical practitionersInt J Chron Obstruct Pulmon Dis 2011; 6: 659-667
- Arnold E, Bruton A, Ellis-Hill CAdherence to pulmonary rehabilitation: A qualitative studyRespir Med 2006; 100: 1716-1723
- Benzo R, Wetzstein M, Neuenfeldt P, McEvoy CImplementation of physical activity programs after COPD hospitalizations: Lessons from a randomized studyChron Respir Dis 2015; 12: 5-10
- Fischer MJ, Scharloo M, Abbink JJ, van 't Hul AJ, van Ranst D, et alDrop-out and attendance in pulmonary rehabilitation: the role of clinical and psychosocial variablesRespir Med 2009; 103: 1564-1571
- Garrod R, Marshall J, Barley E, Jones PWPredictors of success and failure in pulmonary rehabilitationEur Respir J 2006; 27: 788-794
- Harris D, Hayter M, Allender SImproving the uptake of pulmonary rehabilitation in patients with COPD: Qualitative study of experiences and attitudesBr J Gen Pract 2008; 58: 703-710
- Keating A, Lee A, Holland AEWhat prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic reviewChronic Respir Dis 2011; 8: 89-99
- Overington JD, Huang YC, Abramson MJ, Brown JL, Goddard JR, et alImplementing clinical guidelines for chronic obstructive pulmonary disease: Barriers and solutionsJ Thor Dis 2014; 6: 1586-1596
- Perez X, Wisnivesky JP, Lurslurchachai L, Kleinman LC, Kronish IMBarriers to adherence to COPD guidelines among primary care providersRespir Med 2012; 106: 374-381
- Fischer MJ, Scharloo M, Abbink JJ, Thijs-Van A, Rudolphus A, et alParticipation and drop-out in pulmonary rehabilitation: A qualitative analysis of the patient's perspectiveClin Rehabil 2007; 21: 212-221
- Seymour JM, Moore L, Jolley CJ, Ward K, Creasey J, et alOutpatient pulmonary rehabilitation following acute exacerbations of COPDThorax 2010; 65: 423-428
- Høgsgaard Andersen J TT, Kousgaard MBPraktiserende læger savner viden om de kommu-nale sundhedstilbud : Viser ny undersøgelse fra Forskningsenheden for Almen Praksis i KøbenhavnTidsskr Dan Sundhedsvæsen 2015; 91
- Johnston KN, Young M, Grimmer KA, Antic R, Frith PABarriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: A qualitative studyPrimary Care Respir J 2013; 22: 319-324.

