Awad Magbri*, Eussera El-Magbri and Mariam El-Magbri
Dialysis Access Center of Pittsburgh, PA, USA
*Corresponding Author:
Awad Magbri
MD, FACP
Dialysis Access Center of Pittsburgh
PA, USA
Tel: 4122715106
E-mail: elmagbri@hotmail.com
Received Date: October 22, 2017; Accepted Date: October 30, 2017; Published Date: November 10, 2017
Citation: Magbri A , El-Magbri E, El- Magbri M (2017) Whe n Arterial, Venous Pressure and Blood Flo w are Deceiving Compared to Physical Examination and Arterial-Venous Fistula Angiogram. Acta Psychopathol 3:76. doi: 10.4172/2469-6676.100148
Keywords
Arterial pressure; Venous pressure; End-stage renal disease; Hemodialysis; Arterial-venous fistula; Stenosis; Access; Surveillance; Angiogram; Aneurysm of the fistula
Introduction
The case is 68 year old African American female with history of type-2 diabetes mellitus, hypertension, congestive heart failure (CHF), hyperlipidemia, and end-stage renal disease (ESRD) on hemodialysis (HD) for 8 years via a left radial-cephalic arterial venous fistula (RCAVF). She was referred to the dialysis access center of Pittsburgh, PA for evaluation of her RCAVF because of tense lower aneurysm but no bleeding or high venous pressure recordings. Here blood flow on HD ranges from 550-600 ml/ min, with venous pressure range of 81-201mmHg. The venous access pressure ratio (VAPR) with the graph is shown in Graph 1. She had a total of 8 interventions (angioplasties) on her fistula because of stenosis in the draining cephalic vein between the 2 aneurysms. The dialysis nurse is cannulating her below and above the stenotic area with no increase of her venous pressure or decrease in her blood flow, see the angiogram pictures (Figures 1 and 2). We presented this case to show the deceiving venous, arterial pressure and blood flow had physical examination and angiogram of the fistula were not done. This case illustrated the shortcoming of the access surveillance using pressure and blood flow measures if not supplemented with physical examination of the access.
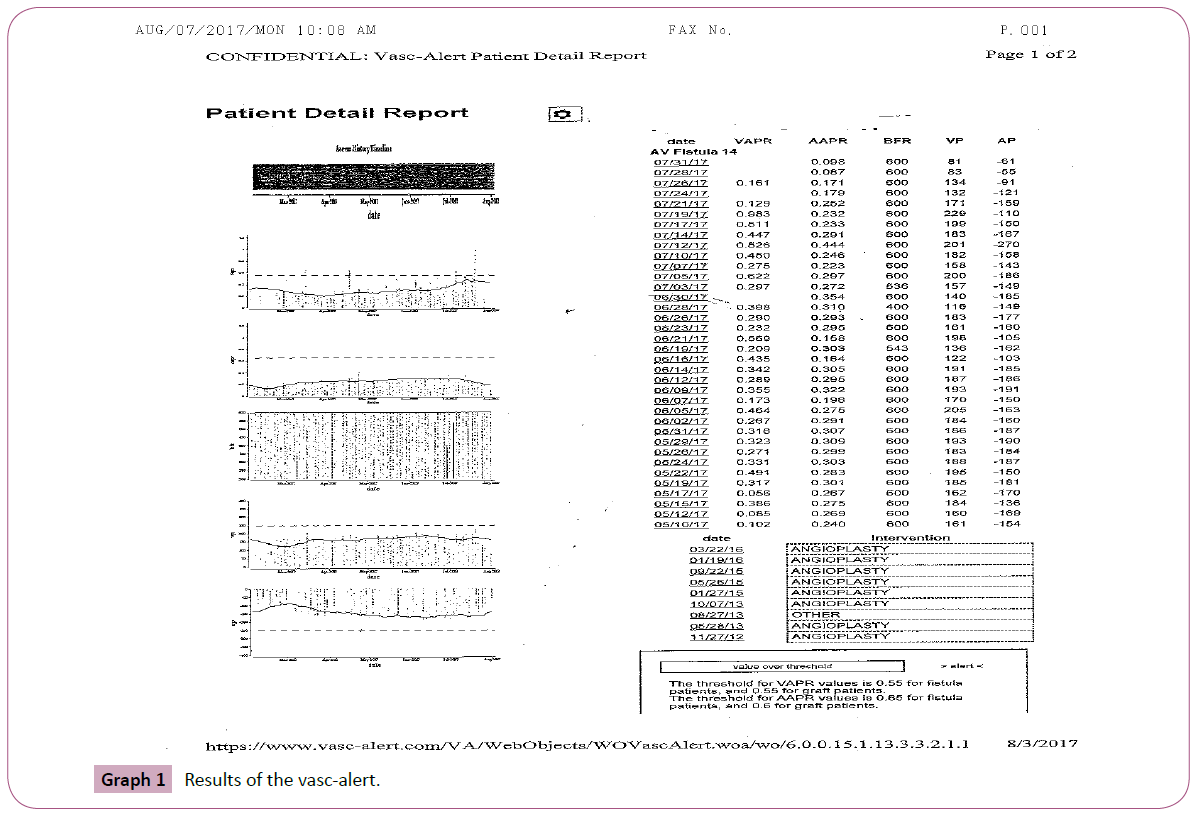
Graph 1: Results of the vasc-alert.
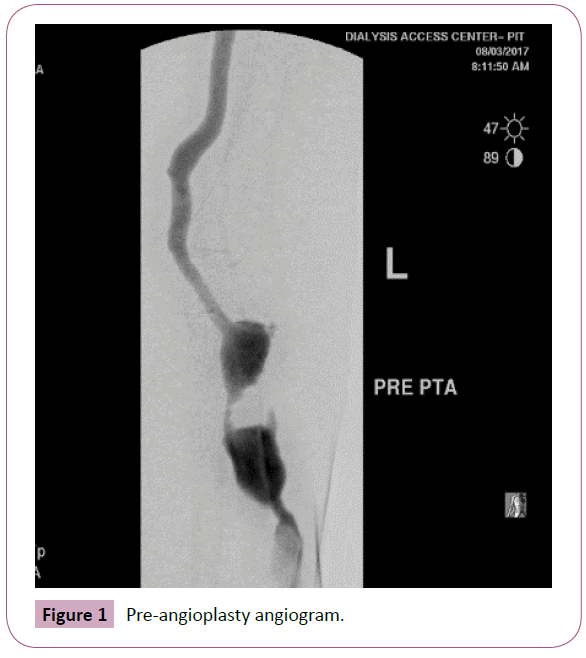
Figure 1: Pre-angioplasty angiogram.
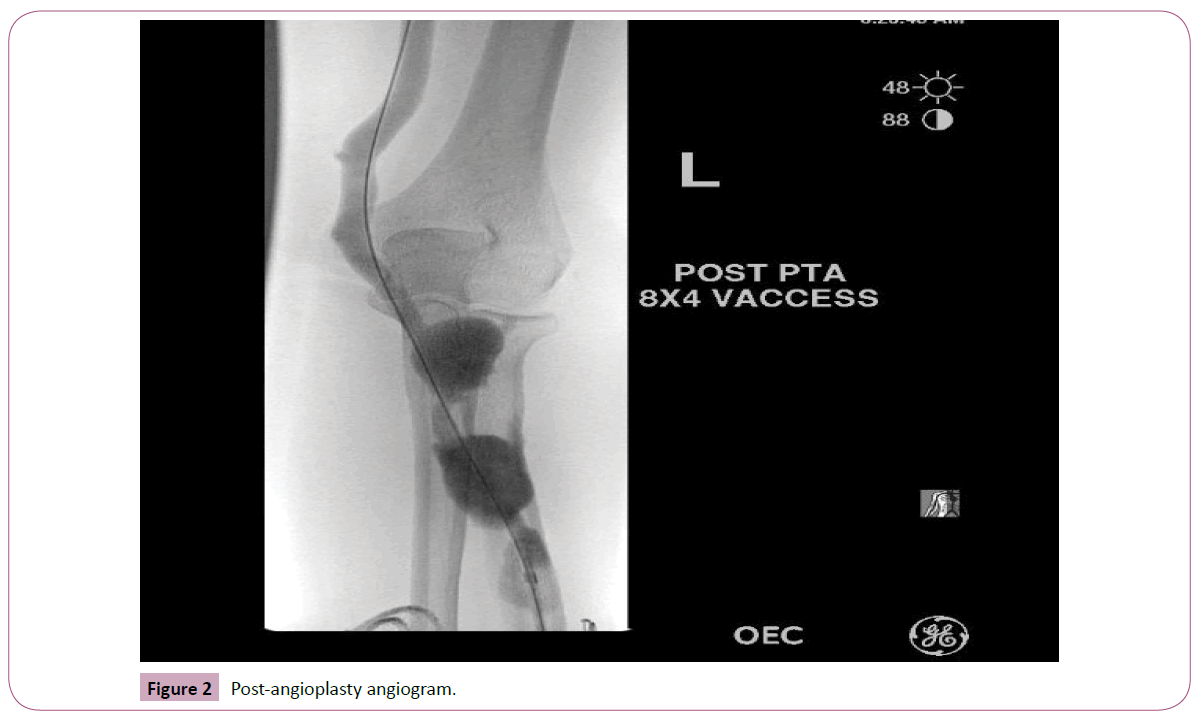
Figure 2: Post-angioplasty angiogram.
Discussion
Access surveillance is important to prevent access dysfunction and decrease access complication (stenosis and thrombosis). These are the most common reasons of hospitalization in end-stage renal disease patients. Stenosis refers to the reduction in the diameter of the access which impedes flow through the access. This is usually due to neo-intimal hyperplasia induced by trauma and turbulent blood flow [1-3]. Significant stenosis in the access leads to ineffective dialysis with decrease life of access [4] and eventually, hypertension with its attending complications. Two methods are used for access surveillance, direct method with Doppler ultra-sound or Magnetic resonance angiography where the degree of blockage is measured by the degree of access stenosis. These methods are expensive and cannot be performed in regular dialysis sessions [5,6].
On the other hand, the indirect measurement do not provide any information about the access diameter. However, they measure the rate of flow through the access and the pressure at different points in the access [5-10]. Low flow rate and high access pressure indicate access stenosis at some location up-stream to the point of measurement. These methods are inexpensive as flow rate or pressure readings can be obtained directly from the dialysis machine. The indirect measures are most popular in access surveillance. The ratio of access pressure to the mean arterial pressure (VAPR) measured during each dialysis is used in our centers for surveillance. The current recommendations by the National Kidney Foundation (KDOQI threshold) suggested intervention for all patients when the VAPR hits a value of 0.55. It is well known that stenosis reduces the life of the access and decrease the effectiveness of HD (4). Timely intervention is beneficial to the quality of life for patients with ESRD [4,11]. The relationship between the blood flow through the access and the stenosis is sigmoidal and hence, blood flow remains unchanged with progression of stenosis (60%) until critical stenosis is reached when flow decreases precipitously.
We used on line software (Vasc-Alert) that measures blood flow, arterial and venous pressures and (VAPR, AAPR) in real time during dialysis. The threshold for VAPR values is 0.55 for fistula patients, and 0.55 for graft patients. The threshold for AAPR values is 0.65 for fistula patients and 0.6 for graft patients. The system gives alert warning and after 3 alerts the patients should be send for angiogram of their access. The data is also graphically displayed for ease of interpretations. However in this case the data were normal and showed no alert warning because the needles are placed in a way that bypass the stenosis. If it was not because of the history and physical examination of the access we could missed the significant stenosis. It is highly recommended that history and examination of the access should be an integral part of access monitoring.
References
- Grajdeanu PB, Schugart RC, Friedman A, Valentine C, Agarwal AK, et al. (2008) A mechanical model of venous neo-intimal hyperplasia formation. Theor Biol Med Model 5: 2-10.
- Roy-Chaudhury P, Kelly BS, Miller MA (2001) Venous neo-intimal hyperplasia in polytetrafluoroethylene dialysis grafts. Kidney Int 59: 2325-2334.
- Sukhatme V (1996) Vascular access stenosis: prospects for prevention and therapy. Kidney Int 46: 1161-1174.
- National Kidney Foundation (2001) KDOQI clinical practice guidelines for vascular access. Am J Kidney Disease 37: S137- S181.
- McDougal G, Agarwal R (2001) Clinical performance characteristics of hemodialysis graft monitoring. Kidney Int 60: 762-766.
- Paulson WD, Ram SJ, Work J (2001) Use of vascular access blood flow to evaluate vascular access. Am J Kidney Disease 37: 451-452.
- Besarab A, Lubkowski T, Frinak S, Ramanathan S, Escobar F (1997) Detection of access strictures and outlet stenosis in vascular accesses: which test is best? ASAIO J 43: 543-547.
- Besarab A, Sullivan KL, Ross R, Moritz M (1995) The utility of intra-access monitoring in detecting and correcting venous outlet stenosis prior to thrombosis. Kidney Int 47: 1364-1373.
- Frinak S, Zasuwa G, Dunfee T, Besarab A, Yee J (2002) Dynamic venous access pressure ratio test for hemodialysis access monitoring. Am J Kidney Diseases 40: 760-768.
- Plantinga LC, Jaar BG, Astor B, Fink NE, Eustace JA, et al. (2006) Association of clinic vascular access monitoring practices with clinical outcomes in hemodialysis patients. Nephron Clin Pract 104: 151-159.
- Schwab SJ, Raymond JR, Saeed M, Newman GE, Dennis PA, et al. (1989) Prevention of hemodialysis fistula thrombosis, early detection of venous stenosis. Kidney Int 36: 707-711.

