Keywords
Death; Culture; Belief; Attitude; Environment; Health; Religion Africa; Nigeria
Introduction
Since Wing proposed the concept of Asperger’s syndrome in 1981 [1], Asperger’s syndrome has garnered attention, and the number of diagnoses of pervasive developmental disorders (PDDs) including Asperger’s syndrome has continued to increase. In recent clinical practice, rather than categorical judgments of whether certain symptoms represent a specific disease, these symptoms have been placed on a continuum known as Autism Spectrum Disorder (ASD), with the continuous transition of severity from normal to severe.
Clinically, it has been suggested that many adults with mental disorders have undiagnosed ASD [2-4]. In Japan, the prevalence of ASD in child was 0.16-0.2% in 2005 [5,6] and 4.8% in the survey in 2012 [7]. Although there is also a change in the concept, there is a possibility that the prevalence of ASD in Japan is increasing. The prevalence of ASD in adults was first reported in the U.K in 2007 as approximately 1% of the population [4,8] though it is believed that many potential ASD patients remain undiagnosed and the comorbidities (secondary disorders) remain untreated. The prevalence of adult ASD in Japan has not been reported yet.
Although health and education services for children with ASD are relatively well established, service provision for adults with ASD is in its infancy [9]. There is a lack of health services research for adults with ASD [10-13], including the identification of comorbid health difficulties, rigorous treatment trials, the development of new pharmacotherapies, and gender differences.
Many college students with mental problems come to our health service center for consultation, and we have found that there are ASDs in their histories. Did they have signs of maladjustment before adolescence? Concerning the history of ASD, are there gender differences? We hypothesized that if ASD received supports at an early stage, they may not be maladapted in adulthood, and that girls are less receiving supports because of less conspicuous.
We wanted to assess whether there were evident signs in the early stage of the disease. We examined the possibility of early intervention by focusing on psychiatric or psychosomatic symptoms in early childhood and assessed the transition of these symptoms in subjects presenting adolescent ASD.
Methods
Subjects and methods
This study included 97 students with ASD (56 males and 41 females) who visited psychiatrists between 2005 and 2016. The average age of the patients was 22.3 ± 3.2 years.
First, we retrospectively investigated the presence of current comorbidities and noted histories of mental problems. We also retrospectively examined the transformation of psychosomatic symptoms during adolescent development in the entire cohort; however, of the 97 subjects, we were able to obtain detailed childhood medical histories for only 62 subjects. In this subset of subjects, we also investigated the incidences of consultations, treatment, and support (n=62, 35 males and 27 females).
Analysis
Comparisons were performed using the chi-squared test; P<0.05 was considered statistically significant. SPSS (IBM Corporation, Armonk, NY) was used for statistical analyses.
Ethical considerations
All protocols in this study complied with the ethics standards of the relevant national and institutional committees on human experimentation, and with the Declaration Helsinki of 1975, as revised in 2008. This study was approved by the Ethics Committee of Hiroshima University (No: E-774), Hiroshima, Japan.
Results
Current comorbidity
We performed the Japanese version of the Autism-Spectrum Quotient-Japanese version (AQ-J) in the 62 patients. The AQ is a questionnaire published by Baron-Cohen [14,15] to investigate the autism spectrum tendency for adults. It consists of 50 statements, and the patients’ average score was 30.1 ± 6.5 points.
Their comorbidities are shown in Table 1. Mood disorders were the most frequent, being observed in 22 subjects (35%), followed by anxiety disorders in 10 subjects (16%), adjustment disorders in 8 subjects (13%), eating disorders in 8 subjects (13%), and somatoform disorders in 6 subjects (10%).
| Comorbidity |
Case (%) |
| Mood disorders |
22 (35.5) |
| Anxiety disorder |
10 (16.1) |
| Adjustment disorder |
8 (12.9) |
| Eating disorder |
8 (12.9) |
| Somatoform disorder |
6 (9.7) |
| Obsessive-compulsive disorder |
4 (6.5) |
| Schizophrenic disorder |
3 (4.8) |
| Others |
1 (1.6) |
Note: The students’ comorbidities are shown. Mood disorders were the most frequent (N=22, 35.5%).
Table 1: Current comorbidity.
The transformation of symptoms from childhood
The transformation of symptoms in the 62 patients, whose information from early childhood was available, is shown in Figure 1. Many patients (34 patients; 55%) showed psychosomatic symptoms during their childhood. Twenty-five of these subjects (25/34, 74%) showed psychosomatic symptoms during their early childhood that persisted until their adolescence. However, in 9 patients (26%), childhood psychosomatic symptoms changed to mood disorders or eating disorders during adolescence.
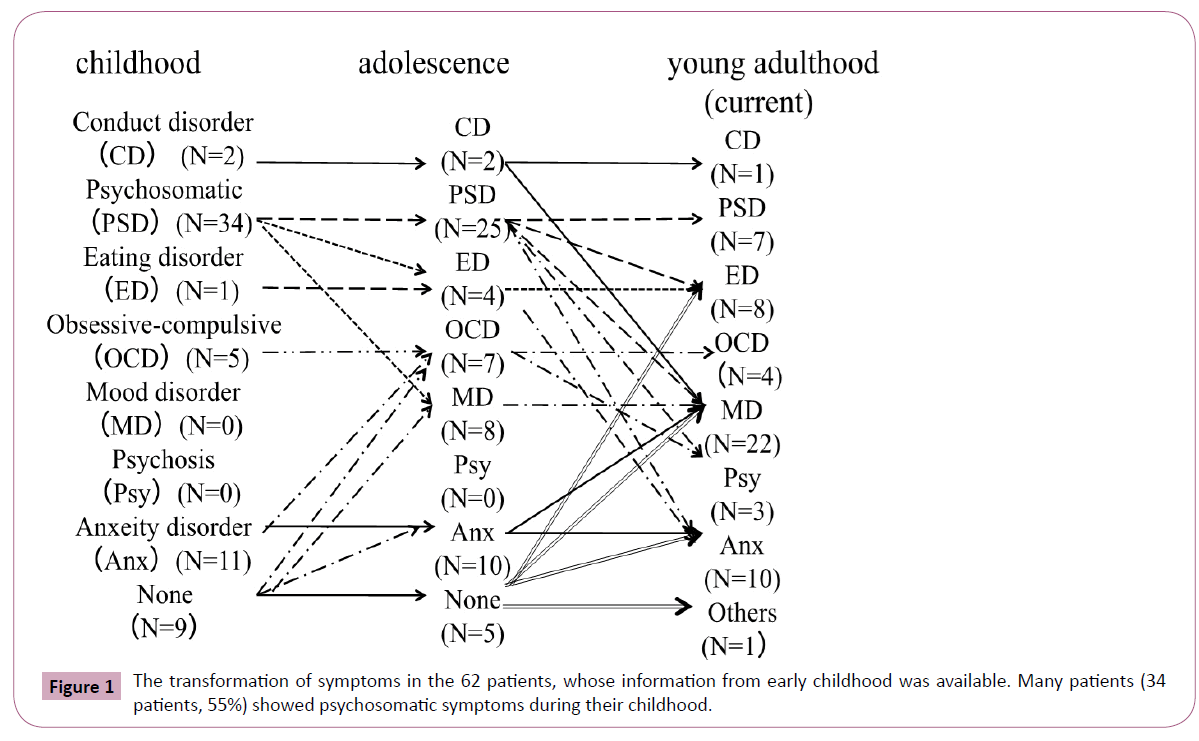
Figure 1: The transformation of symptoms in the 62 patients, whose information from early childhood was available. Many patients (34 patients, 55%) showed psychosomatic symptoms during their childhood.
Of these 25 cases with psychosomatic symptoms in adolescence, only 7 cases remained psychosomatic symptoms in young adulthood. Eighteen cases (18/25, 72%) changed to mood disorders, eating disorders, anxiety disorders, or psychotic symptoms in young adulthood.
The psychosomatic symptoms in early childhood were diverse, including gastrointestinal symptoms such as nausea, vomiting, and anorexia, in addition to orthostatic dysregulation, headache, asthma, and allergic symptoms.
Comparisons of having problems or not in childhood and adulthood
The comparisons of having problem or not in childhood and adulthood are shown in Table 2. In childhood, there were significantly more cases with psychosomatic symptoms, whereas in young adulthood, there were significantly more cases with other symptoms (anxiety, obsession, others) (χ2(2)=44.3, p<0.01).
| Symptoms |
Childhood |
Young adulthood |
χ2 |
φ |
| None |
9** |
0 |
44.3 |
0.60 |
| Psychosomatic symptoms |
34** |
7 |
|
|
| Others |
19 |
55** |
|
|
**P <0.01
Note: The comparisons of having problem or not in childhood and young adulthood are shown. In childhood, there were significantly more cases with psychosomatic symptoms (P<0.01). In young adulthood, there were significantly more cases with other symptoms (P<0.01).
Table 2: Comparison of having problems or not in childhood and adulthood.
Male and female comparisons of symptoms in childhood
The male and female comparisons of symptoms in childhood are shown in Table 3. Females had significantly more psychosomatic symptoms (χ2(2)=7.19, p<0.01).
| Symptoms |
Male N (%) |
Female N (%) |
χ2 |
φ |
| None |
7 (20) |
2 (7.4) |
7.19 |
0.34 |
| Psychosomatic symptoms |
14 (40) |
20 (74.1)** |
|
|
| Others |
14 (40) |
5 (18.5) |
|
|
**P<0.01
Note: The male and female comparisons of symptoms in childhood are shown. Female had significantly more psychosomatic symptoms (P<0.01).
Table 3: Symptoms in childhood: comparisons of male and female.
Psychosomatic symptoms during adolescence
Adolescence is a period of time when changes in symptoms easily occur; thus we investigated the changes in psychosomatic symptoms. Figure 2 shows the transformation of the psychosomatic symptoms during adolescence. In adolescence, psychosomatic disorders of the digestive system such as irritable bowel syndrome (IBS) were the most commonly observed, with 11 subjects presenting such disorders (44%), followed by hyperventilation syndrome in 5 subjects (20%), and eating disorders in 4 subjects (16%). Among the 11 subjects with IBS, digestive symptoms persisted in 4 subjects. The symptoms changed to mood or anxiety disorder or to eating disorder. Hyperventilation syndrome changed to mood or anxiety disorder. Eating disorders persisted in all cases. In other cases, the symptoms transformed to mood disorders and psychotic symptoms.
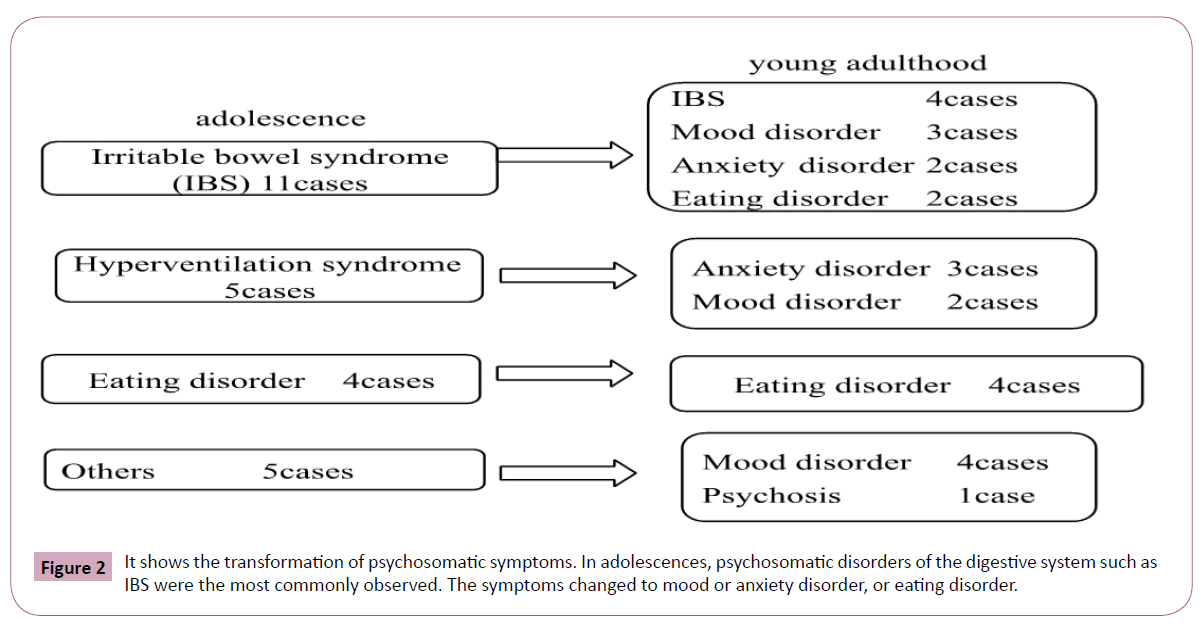
Figure 2: It shows the transformation of psychosomatic symptoms. In adolescences, psychosomatic disorders of the digestive system such as IBS were the most commonly observed. The symptoms changed to mood or anxiety disorder, or eating disorder.
Past treatment/support in childhood
Table 4 shows the male and female comparisons of past treatment or professional support. Significantly more male students and significantly fewer female students had treatment/support in childhood (χ2(1)=9.90, p<0.01).
| Past treatment/support |
Male (cases) |
Female (cases) |
χ2 |
φ |
| Presence |
23** |
6 |
9.90 |
0.40 |
| Absence |
12 |
21** |
|
|
**P <0.01
Note: The male and female comparisons of past treatment or professional support are shown. Significantly more male students had treatment/support in childhood (P<0.01), and significantly more female students had no treatment/support in childhood (P<0.01).
Table 4: Past treatment/support in childhood: comparisons of male and female.
The relationships between the presence of treatment and support in childhood and present adaptability are shown in Table 5. Among the 62 subjects, 18 out of 29 subjects (62%) who received some form of treatment in childhood were able to adapt to college life, whereas only 9 out of 33 subjects (27%) who did not receive treatment were able to adapt to college life. There were significantly more cases of favorable adaptation in the subjects who received treatment (χ2(1)=6.52, p<0.01).
| Current adjustment |
Past treatment/support |
χ2 |
φ |
| Presence (cases) |
absence (cases) |
| Good adjustment |
18** |
9 |
6.52 |
0.32 |
| Maladaptation (school refusal, et al.) |
11 |
24** |
|
|
**P <0.01
Note: The relationship between the presence of treatment/support in childhood and present adaptability are shown. There were significantly more cases of good adaptation in the students who received treatment/support (P<0.01).
Table 5: Association between past treatment/support and current adaptation.
Discussion
Comorbidity with ASD
Certain problematic symptoms in adulthood are not an exacerbation of underlying developmental disorders but, instead, the occurrence and exacerbation of comorbid mental disorders. Previously, we also investigated the relationship between ASD and the mental health of college students, reporting that in college students with ASD, normal coming-of-age identity crises and environmental changes such as college entrance examinations were risk factors for the development of secondary disorders [16,17]. Regarding secondary disorders, many previous studies, such as that by Tantam et al., have reported that depression is the most common disorder and that its prevalence becomes higher as age increases [18,19]. Other reports have said that adults with ASD have significantly increased rates of mental health problems, including mood and anxiety disorders, obsessive-compulsive disorder, and psychotic disorders [10,20,21]. Our results also show that mood disorders are the most common comorbid disorder, followed by anxiety disorders. The free environment of a university can sometimes decrease the protective frameworks for these students, thereby threatening their sense of security.
Predictably, some type of setback experience (the collapse of a relationship with others, problems in report submission, failure obtaining a job, etc.) can cause depression.
Transformation of psychosomatic symptoms and other symptoms
To address whether any underlying/undiagnosed ASD existed in students who consulted psychiatrists and whether there was a possibility of earlier intervention, we conducted a survey regarding the symptoms observed in childhood. The results demonstrated that many subjects (33 cases; 58%) showed psychosomatic symptoms in childhood. It is believed that children are likely to develop psychosomatic symptoms due to incomplete mental and physical development and a susceptibility to environmental influences.
In 1972, Sifneos introduced the concept of “alexithymia,” a personality that is likely to cause psychosomatic disorders [22]. Alexithymia is characterized by a lack of awareness of internal feelings and conflicts and poor self-reflection. Similarly, in interpersonal relationships, these patients have difficulty in empathic communication; thus, it has characteristics that are common with ASD, including Asperger’s syndrome. In ASD, although there is a unique hypersensitivity to somato-sensation, there is also insensitivity to proprioception, suggesting that psychosomatic symptoms are more likely to develop.
Investigating the transformation of psychosomatic symptoms in childhood, it is evident that the symptoms change from a variety of physical symptoms in childhood to specific (organ selective) symptoms, depression and anxiety in adolescence. The symptoms emerge as physical symptoms in childhood due to low stress tolerance and the immaturity of emotional processing, and many of these patients subsequently develop emotional symptoms in adolescence. Woodman et al report a transformation of symptoms during adolescence in patients with ASD [23]. Adolescence is the period in which various psychological burdens can occur because of physical changes, encountering other people’s opinions, the recognition of being different, and the pressures of examinations and study, resulting in various psychiatric symptoms such as exacerbation of depression, anxiety, and obsessive symptoms. Although some people develop these disorders without any pre-existing conditions, it is also possible that some of these patients had psychosomatic symptoms in childhood and subsequently developed other psychiatric symptoms during adolescence, as observed in our subjects.
Eating disorders persisted from adolescence to young adulthood. When Wing proposed the concept of Asperger’s syndrome in 1981, its association with eating disorders was established [1]. Huke reviews the prevalence of eating disorders associated with ASD and reports eating disorders in 22.9% of ASD patients. In particular, the relationship between ASD and anorexia nervosa (AN) has been indicated [24]. There are many common characteristics, such as obsessive-compulsiveness, persistence, poor cognitive flexibility, and difficulty in interpersonal relationships. Furthermore, there are many common neural abnormalities related to the “social” areas of the brain (e.g., the amygdala and the anterior cingulate gyrus) [25]. ASD can actually be the cause of an eating disorder because of isolation from groups and lack of self-evaluation. Eating disorders tend to be chronic, and they can be particularly severe if symptoms occur to compensate for negative self-evaluation.
Gender differences in symptoms in childhood
Many reports have suggested that ASD occurs more commonly in males than in females, with gender ratios of 4.3:1 [26,27] and 3.3:1 [28], among others. Mandy says that ASD may present differently in females than in males; thus, females are often under-diagnosed or mislabelled [29]. Females with ASD have better social skills than their male counterparts [30], are less likely to have externalizing behaviors, such as hyperactivity/ impulsivity and behavioral problems, and are more vulnerable to internalizing problems, such as anxiety, depression, and eating disorders [24,31]. Bargiela reports on females with ASD diagnosed in late adolescence or adulthood and provides in-depth accounts of “pretending to be normal” [32].
In this study, males had cases with behavioral problems in childhood, but females did not. Both males and females had cases with anxiety in childhood. Males had significantly more cases with psychiatric symptoms with behavioral disorders, whereas females had significantly more psychosomatic symptoms in childhood. We found that females in particular had psychosomatic symptoms that changed to psychiatric symptoms such as depression and eating disorders.
The relationship with adaptability in adolescence
According to our investigation of adaptability in adolescence, many subjects who received treatment during childhood went on to be very adaptable in college whereas many of the maladapted subjects did not receive treatment. These results suggest that when there is some form of treatment and/or support during childhood in patients with psychosomatic symptoms, favorable effects are long lasting. Intervention in students with psychosomatic symptoms in elementary and middle school may lead to the prevention of secondary disorders. School nurses, teachers, and school doctors are often the first persons approached for consultation. Regarding physical symptoms in students, the results show that it may be important to consider the relationship with stress and environment for somato-autonomic integration.
There is an increasing recognition of the need for young people with neurodevelopmental disorders to have a transition from child to adult health services [9,33-36]. The significant point is the persistence of psychiatric problems from childhood to adulthood. In ASDs, when symptoms occur at infancy, it is necessary to consider strategies that may allow the patient to avoid the persistence of secondary disorders into adulthood. It is important to provide educational and social interventions based on the life plan of the child without over-adaptation or over-expectation. When psychosomatic symptoms present, many patients are in fact over-stressed due to over-intervention. However, when intervention is not provided to the child because of an absence of obvious maladaptation, problems may be exacerbated in adulthood, thereby increasing the possibility for secondary disorders.
In subjects who received continuous treatment or support during childhood, favorable adaptation occurred at a subsequent stage. Many subjects had not undergone continuous treatment, suggesting that to prevent secondary disorders, it may be important to continue treatment based on a long-term perspective to avoid future problems.
Tanaka discusses changes due to development, and when children with ASD face difficulties in balancing their childish understanding with reality, it is possible that self-image is impaired by common negative life experiences, including the many experiences of failure during preschool and the school years in Japan [37]. It is important not to overlook the potential signs of ASD in childhood such as psychosomatic symptoms and to provide treatment or support self-image repair to prevent secondary disorders.
The need for early support
Our study results showed that children with ASD are likely to develop psychosomatic symptoms as stress responses to specific somato-sensation disorders and maladaptation to their surrounding environments. It has been suggested that when appropriate countermeasures are not undertaken, problems become more complicated; for example, psychosomatic symptoms change during growth and development and become more diverse, and emotional problems such as depression and anxiety present in adolescence. Children with ASD are more likely to adopt a crutch when problematic behavior presents. When this occurs, the signs are easily overlooked due to a superficial adaptation (sometimes over-adaptation). When physical symptoms present, the first places for consultation are a pediatric clinic or a nurse’s office in the school. Dysfunctional somato-autonomic integration should be considered when children have functional physical disorders. It is important for the adults around the child to ensure a sense of safety and to adjust the environment based on the potential for stress since it is difficult for young children to both recognize stress and verbalize their emotions. It is likely that long-term maladaptation after adolescence can be avoided by appropriate early diagnosis and support. Consensus guidelines regarding transitions for young adults with special care health needs have been available for the last decade [38]. We hope that such support will increase in the future.
Limitation
The subjects were few in number and were college students who were intellectual and considered to be a relatively good group adaptively; thus, it is difficult to claim that these findings express the ASD perspective.
Conclusion
This study showed that those who received special support during early childhood were better adapted for young adults. From the results, it seemed that early intervention was important for preventing maladaptation. Furthermore, in this study, many young adults with comorbidities had psychosomatic symptoms in childhood, so it was necessary to find psychosomatic symptoms and to intervene in early childhood.
References
- Wing L (1981) Asperger’s syndrome: a clinical account. Psychol Med 11: 115-129.
- Valkanova V, Rhodes F, Allan CL (2013) Diagnoses and management of autism in adults. Practitioner 257: 13-16.
- Kamio Y, Moriwaki A, Takei R, Inada N, Inokuchi E, et al. (2013) Psychiatric issues of children and adults with autism spectrum disorders who remain undiagnosed. Seishin shinkeigaku Zasshi 115: 601-606.
- Brugha TS, McManus S, Bankart J, Scott F, Purdon S, et al. (2011) Epidemiology of autism spectrum disorders in adults in the community in England. Arch Gen Psychiatry 68: 459-465.
- Honda H, Shimizu Y, Imai M, Nitto Y (2005) Cumulative incidence of childhood autism: a total population study of better accuracy and precision. Dev Med Child Neurol 47: 10-18.
- Honda H, Shimizu Y, Misumi K, Niimi M, Ohashi Y (1996) Cumulative incidence and prevalence of childhood autism in children in Japan. Br J Psychiatry 169: 228-235.
- Imai M, Ito Y (2014) Survey of autism spectrum disorder in Yokohama City Western Medical Center. Bulletin Res Rehab 23: 41-46.
- Brugha TS, Spiers N, Bankart J, Cooper SA, McManus S, et al. (2016) Epidemiology of autism in adults across age groups and ability levels. Br J Psychiatry 209: 498-503.
- Murphy CM, Wilson CE, Robertson DM, Ecker C, Daly EM, et al. (2016) Autism spectrum disorder in adults: diagnosis, management, and health services development. Neuropsychiatr Dis Treat 12: 1669-1686.
- Murphy DG, Beecham J, Craig M, Ecker C (2011) Autism in adults: new biological findings and their translational implications to the cost of clinical services. Brain Res 1380: 22-33.
- Howlin P, Moss P (2012) Adults with autism spectrum disorders. Can J Psychiatry 57: 275-283.
- Shattuck PR, Roux AM, Hudson LE, Taylor JL, Maenner MJ, et al. (2012) Services for adults with an autism spectrum disorder. Can J Psychiatry 57: 284-291.
- Pellicano E, Dinsmore A, Charman T (2014) What should autism research focus upon? community views and priorities from the United Kingdom. Autism 18: 756-770.
- Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E (2011) The Autism-Spectrum Quotient (AQ): Evidence from Asperger syndrome/ high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 31: 5-17.
- Wakabayashi A, Baron-Cohen S, Wheelwright S, Tojo Y (2006) The Autism-Spectrum Quotient (AQ) in Japan: a cross-cultural comparison. J Autism Dev Disord 36: 263-270.
- Miyake Y,Okamoto Y, Kurosaki M (2011) Pervasive developmental disorders in campus mental health (1) background and secondary psychiatric symptoms. Bulletin of General Health Research, Hiroshima University Health Service Center 27: 9-14.
- Okamoto Y, Miyake Y, Kurosaki M (2011) Pervasive developmental disorder in campus mental health (2) changes of secondary symptoms and approaches from a point of view of resilience. Bulletin of General Health Research, Hiroshima University Health Service Center 27: 15-22.
- Tantam D (1998) Aspreger’s syndrome. J Child Psychol Psychiatry 29: 245-253.
- Ghaziuddin M, Ghaziuddin N, Greden J (2002) Depression in persons with autism: implication for research and clinical care. J Autism Dev Disord 32: 299-306.
- Hofvander B, Delorme R, Chaste P, Nydén A, Wentz E, et al. (2009) Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry 9: 35.
- Lugnegard T, Hallerback MU, Gillberg C (2011) Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res Dev Disabil 32: 1910-1917.
- Sifneos PE (1996) Alexithymia: past and present. Am J Psychiatry 153: 137-142.
- Woodman AC, Smith LE, Greenberg JS, Mailick MR (2016) Contextual factors predict patterns of change in functioning over10 years among adolescents and adults with autism spectrum disorders. J Autism Dev Disrord 46: 176-189.
- Huke V, Turk J, Saeidi S, Kent A, Morgan JF (2013) Autism spectrum disorders in eating disorder populations: a systematic review. Eur Eat Disord Rev 21: 345-351.
- Milosavljevic B, Carter Leno C, Simonoff E, Baird G, Pickles A, et al. (2016) Alexithymia in adolescents with autism spectrum disorder: its relationship to internalising difficulties, sensory modulation and social cognition. J Autism Dev Disord 46: 1354-1367.
- Fombonne E (2003) Epidemiological surveys of autism and other pervasive developmental disorders: An update. J Autism Dev Disord 33: 365-382.
- Fombonne E (2009) Epidemiology of pervasive developmental disorders. Pediatr Res 65: 591-598.
- Mills R, Kenyon S (2013) Autism in pink: prevalence study of females with autism in four participating countries.
- Mandy W, Tchanturia K (2015) Do women with eating disorders who have social and flexibility difficulties really have autism? Mol Autism 6: 6.
- Head AM, McGillivray JA, Stokes MA (2014) Gender differences in emotionality and sociability in children with autism spectrum disorders. Molecular Autism 5: 19.
- Mandy W, Chilvers R, Chowdhury U, Salter G, Seigal A, et al. (2012) Sex differences in autism spectrum disorder: Evidence form a large sample of children and adolescents. J Autism Dev Disord 42: 1305-1313.
- Bargelia S, Steward R, Mandy W (2016) The experiences of late-diagnosed women with autism spectrum conditions: An investigation of the female autism phenotype. J Autism Dev Disord 46: 3281-3294.
- Stewart D (2009) Transition to adult services for young people with disabilities: current evidence to guide research. Dev Med Child Neurol 51: 169-173.
- Young S, Murphy CM, Coghill D (2011) Avoiding the ‘twilight zone’: recommendations for the transition of services from adolescence to adulthood for young people with ADHD. BMC Psychiatry 11: 174.
- www.nice.org.uk/guidance/cg170/resources/guidance-autism NICE
- Cheak-Zamora NC, Yang X, Farmer JE, Clark M (2013) Disabilities in transition planning for youth with autism spectrum disorder. Pediatrics 131: 447-454.
- Tanaka T (2011) The changes of PDD symptoms according to their mental growth. Psychiatria et neurologia Japonica 113: 1123-1129.
- American Academy of Pediatrics, American Academy of Family Physicians, American College of Physicians-American Society of Internal Medicine (2002) A consensus statement on health care transitions for young adults with special health care needs. Pediatrics 110: 1304-1306.

